
 Impressions are key information between Dentist and Dental Labs across the world to transfer reproducible information of the patients mouth since the mid 1800’s. In my time I have found the clinical and technical work is usually of a high standard but why do we have remakes? It’s usually the impression itself. As a commercial dental laboratory we see 1000’s of impressions weekly. We can only see the physical factors of the impression not the representation of the true I/O information as we do not have access to the I/O of the patient so we cannot judge if the impression is true or false. Physical factors of an impression:
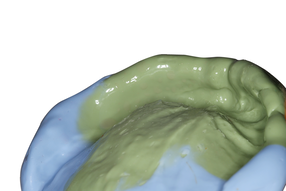
Impression are subjective to cost factors and it’s physical properties which are classed as are elastic or non-elastic materials. Most crown and bridge impressions are taken in the elastomeric category (silicones, PVS, polyethers) and require the following clinical significance to create a true I/O representation of the patients mouth:
All of the above are physical factors is a visual representation of an impression but not a true representation of the I/O of the patient. However, physical factors of an impression increase the risk of variables if not followed correctly and can result in a false representation of the I/O and the only way of controlling the accuracy is chair side:
Physical factors definitions: Overall look A combination of all of physical factors which will provide a visual representation of an impression but not the I/O of the patients mouth. Steps in the impression between material (single or dual phase) Steps in the impression usually occurs when the impression is taken in dual phase and the working times and settings of both impressions materials are not correctly timed. This results in added layer over the prep area that is higher than the adjacent teeth etc this will cause many issues with the restoration. Solution: What we are looking for is a homogeneous mixture of the two material which is achieved by correct mixing, working and setting times: “In chemistry, a mixture is a material made up of two or more different substances which are physically combined. A mixture is the physical combination of two or more substances in which the identities are retained and are mixed in the form of solutions, suspensions and colloids.” Impression through the tray (patient bite through especially on triple tray) Usually occurs in the posterior region, visually seen by holding the impression into a light source. This causes issues in occlusion and false information in the occlusion morphology as the cuspal information is missing with the mesh or tray cutting this information away and dictating a false representation of flat cusps. Solution: Check the tray selection, control and dictate the impression when inserting and do not push hard, keep the impression stable by keeping one index finger and middle finger on each side of the tray with the handle firmly in between the thenar (muscle below the thumb) and ring finger. Only use one hand, the other hand can be used to preform border moulding etc. With full arch impressions, the impression is loaded, inserted and controlled by the dentist who controls and dictates the impression in all aspects which is visually seen by the Dentist. Triple trays are loaded, inserted into the patients mouth and the patient is asked to bite together, which is controlled by the patient, not the Dentist as the dentist cannot visually see intra orally and cannot control or dictate the impression. Triple trays? This is a big topic and I have created it’s own blog for it (click here to view this). Positioning of arch in the tray (prep area too close too plastic tray wall) This occurs when the impression tray selection is not correct or the impression has been incorrectly placed into the patients mouth. This will cause variables and distortion of the physical factors of the impression and restorative areas as the impression capture of the restorative area could be unsupported if it’s out of the tray or if the restorative area is to close to the plastic wall of the tray, this could cause the plastic wall to flex inwards due to it’s reflex memory of the thin plastic and outwards from the impression material itself. Impressions are cast from dental die stone type 3 / 4 in a water to powder ratio form and require a chemical reaction to initiate setting from liquid to solid. The chemical reaction is called an exothermic setting reaction and can reach temperatures of 30 – 45°C within the exothermic reaction, the die stone creates a setting expansion rate (between 0-0.015 to 0.30%) due to outward growth of crystals. Due to nature of die stones reaching temperatures of 30 – 45°C and an expansion rate of 0.15 – 0.30% this will create an expansion against the impression material outwards and in turn the plastic wall of the impression will flex inwards due it’s reflex memory if the restorative area is too close to the plastic. Plastic can be moulded into any shape at 80°C. “Many dual-arch trays currently being used for dual-arch impressions are plastic. Accuracy of our impressions is compromised when these plastic dual-arch trays flex as the impression is taken, which results in consistent discrepancies of 180 to 210 microns. This flex can be caused by the high side walls of the plastic trays hitting the palatal tissues, maxillary tuberosities or tori present in the patient’s oral cavity. Flex can also occur due to outward pressure on the plastic tray when there is interference in the retro-molar pad area. The very act of swallowing during the impression procedure can cause the tongue to repeatedly displace the lingual wall of the tray during polymerization, creating distortion. As well, the thicker rheology of high viscosity impression materials can cause the plastic tray to flex away from the tooth preparation. Therefore, when the tray is removed, the plastic memory of the tray will create an inward pressure, and depending on the stiffness of the heavy body used, the dies can be distorted mesio-distally, creating marginal fit problems as well as interproximal contact issues. Reference: Glidewell Dental, Clinical Predictability with Dual-Arch Impressions: Plastic Trays Are Not the Answer, “Len” Boksman, DDS, B.S., FADI, FICD, Accessed 1st January 2021 (https://glidewelldental.com/education/chairside-dental-magazine/volume-5-issue-1/clinical-predictability-with-dual-arch-impressions-plastic-trays-are-not-the-answer/) In a study published in the Journal of Prosthodontics various impression trays were measured without impression material, on seating and polymerisation of the material and after removing the impression. All tested plastic trays exhibited distortion in cross section and across the arch. Metal trays displayed no distortion. The authors concluded that high viscosity impression materials should not be used with plastic stock trays. (Cho & Chee, 2004) Solution: Check the impression tray selection, try to use a bigger tray to accommodate the arch, make sure the restorative area is aligned in the middle of tray, mould the tray outwards if needed with heat, or add putty to make the tray larger. Trial the impression tray first, use metal stock trays (rim lock trays). Impression material and if adhesive used Impression material faults occur when the impression material chemical properties have not been followed in terms of ratios, temperatures, mixing, working and settings times which results in areas not set correctly and changes the impression detail. This creates false information as drags and pulls in the impression upon removal. Solution: By following the correct ratios, mixing, working and setting times in line with the room temperature will maximise the chemical properties for the physical factors of the impression and limit variables in terms of wettability, flexibility, elastic recovery, tear strength, dimensional stability and detail reproduction within the physical factors of the impression. Adhesive faults occur when the impression material does not seat in the tray after removal which results in a dimensionally unstable impression which distorts both physical factors of the impression and restorative area. This also occurs when the base material of the impression is not pushed firmly enough the tray and results in the impression material coming away from the tray. Solution: Use adhesive in the tray prior to taking the impression to help hold the impression taken after removal in the tray by a chemical reaction. Stock trays have holes for mechanical retention to hold impression material inside of the tray, before insertion firmly pushed the impression into the tray and check underneath the impression to see if there is enough material through the tray. By utilising both mechanical and chemical retention of adhesive will result in physical factors of the impression to be dimensional stable. What our laboratory does to justify it’s quality control (Taken from our terms and condition): Manufacturing of work: We manufacture implant, digital, crown & bridge, prosthetics and orthodontic dental appliances all in-house in London with the exception of full arch titanium implant bars. All materials are sourced from reputable dental companies within the UK. All dental technicians are GDC registered and receive training via the PTC system which helps to ensure uniform standards of quality and technical precision. All work manufactured is quality controlled with department managers preforming the last inspection before despatch. Quality control: With all of our cases we manufacture, we measure out powder/ water ratios for casting impressions and vacuum mix, with all of our denture acrylics we measure out powder / monomer ratios and follow strict guidelines on temperatures, working times and cooling down times from manufactures instructions of the materials to maximise the full chemical and mechanical properties of all our cases manufactured. All of the materials supplied are with in date and any reversible materials disposed off after it’s cycle is complete. All of the impression is cast upon the same day of arrival, after casting the work is checked and signed in. The completed case is signed off by the technician and quality controlled by the department manager before leaving the premises to ensure the parameters (contacts, margin), extension, retention, stability, support & path of insertion are correct. The aesthetics, tooth positioning, occulsion & shade is checked against the RX instructions and notation provided.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Private Dental Laboratory in London
 Kash Qureshi - Managing Director, Clinical Dental Technician Kash Qureshi - Managing Director, Clinical Dental Technician
About the author:
Kash Qureshi is a Clinical Dental Technician (Denturist) in the U.K who oversees and quality controls over 3000+ fixed and removable prosthesis including implant cases from a clinical and technical aspect monthly at Bremadent Dental Laboratory & Swissedent Denture Clinic in London. www.swissedent.co.uk www.bremadent.co.uk [email protected] 
Categories
All
Archives
May 2024
|
 RSS Feed
RSS Feed