
 How to take a denture bite registration for complete dentures?Taking a wax bite registration is a crucial part of fabricating complete dentures, it allows information from the patient to be transferred to the dental laboratory to manufacture a denture based on the patients unique parameters. The information used allows the dental laboratory to provide a tooth set up within the parameters traditionally or CAD, 3D printed. The same information from a wax bite registration applies to both traditional and digital methods of constructing complete dentures. The first stage of any denture case is: Patient details & history, denture history, E/O & I/O examinations, diagnoses, prognosis, treatment options and a treatment plan. How to take bite registration is broken down into 3 steps: Step 1: Orientation Step 2: Facial and smile features Step 3: Register the bite Tools: Fox’s bite plane, rim former, Willis gauge, wax knife, Bunsen burner, PVS dispensing gun Materials: Wax, bite registration paste Functions of a bite registration in complete dentures:
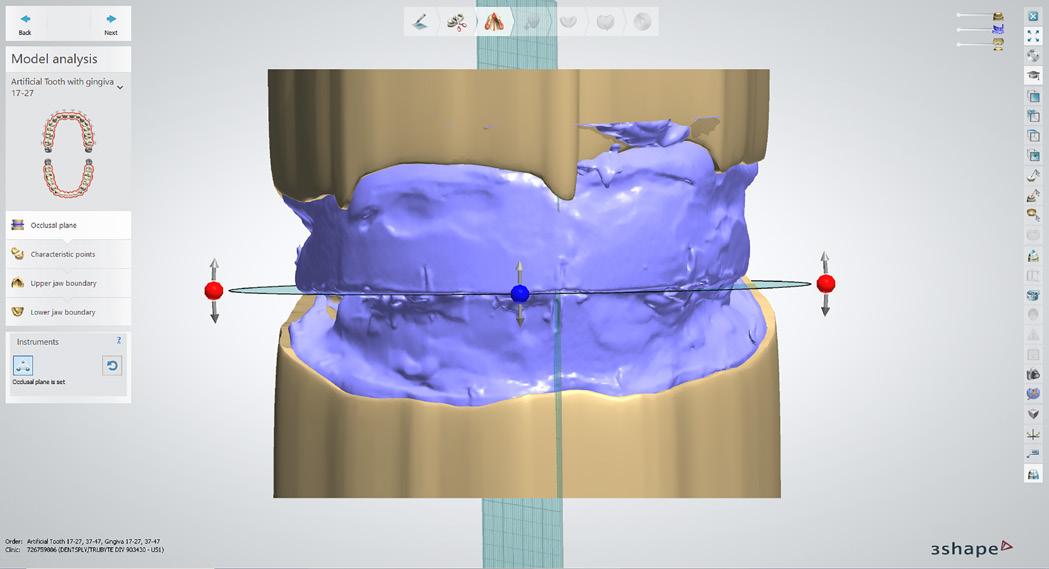
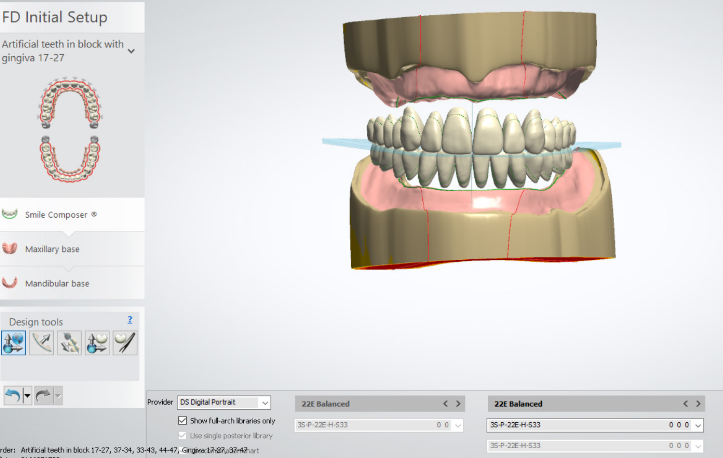
How are wax bite blocks used in digital dentures?
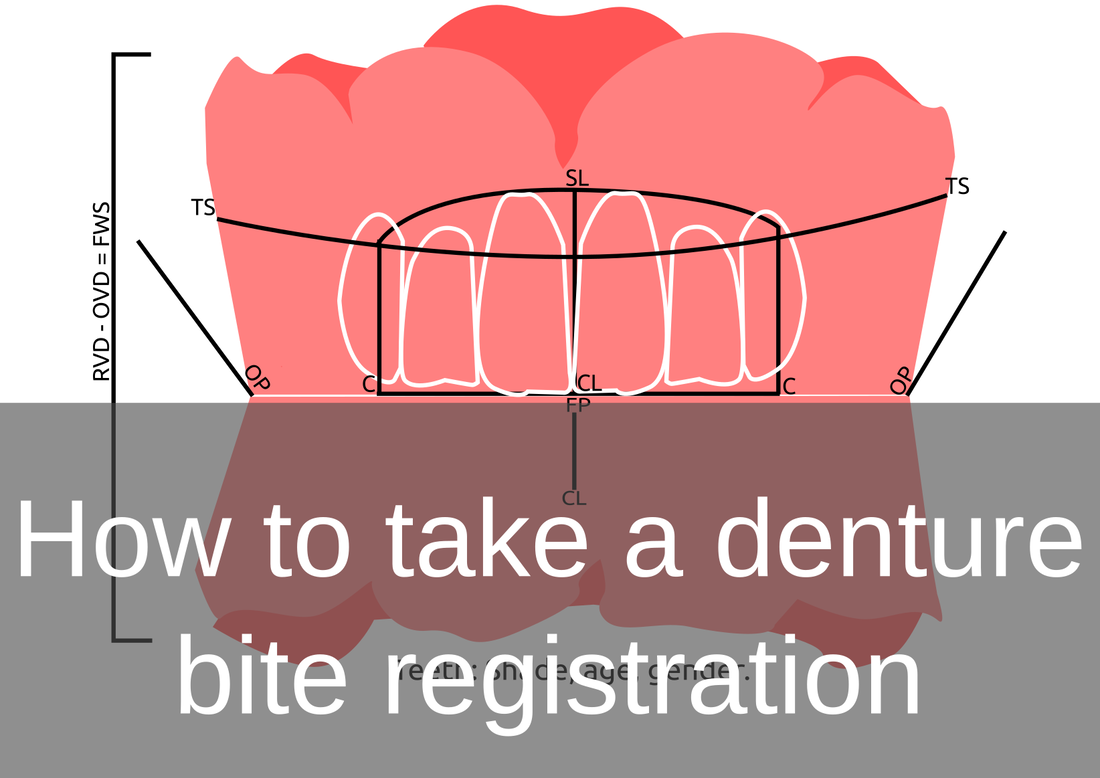
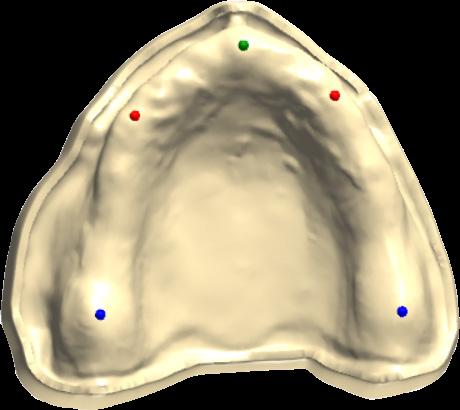
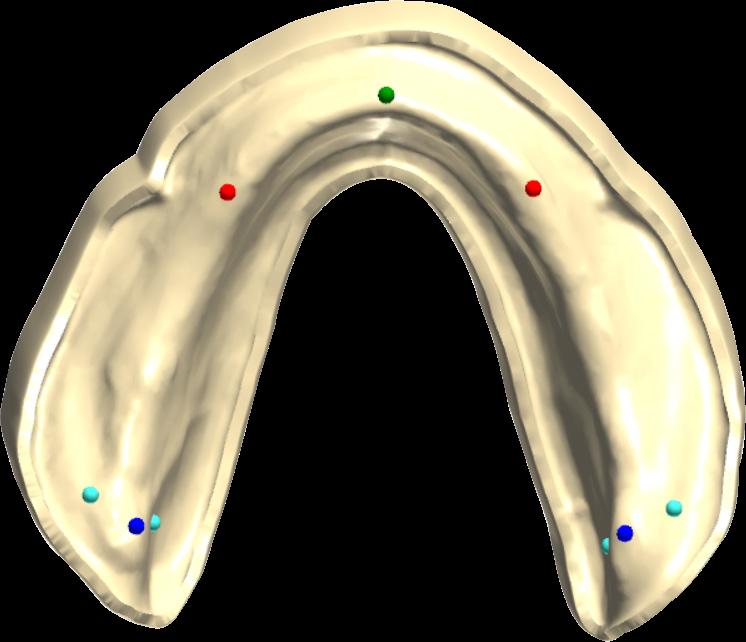
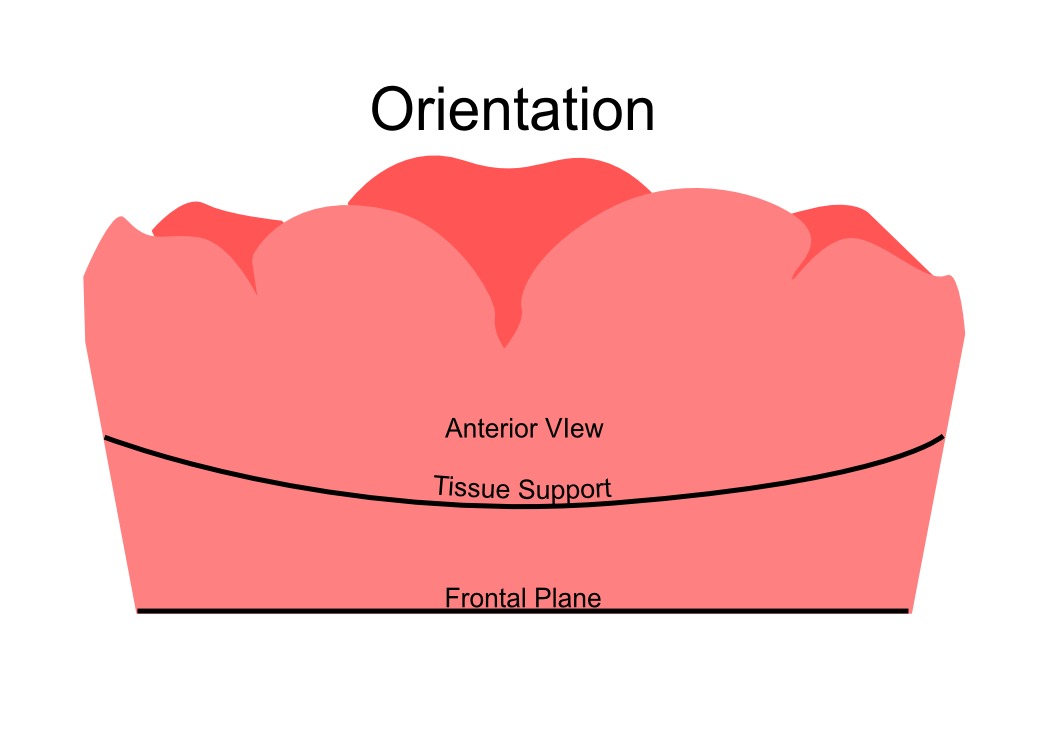
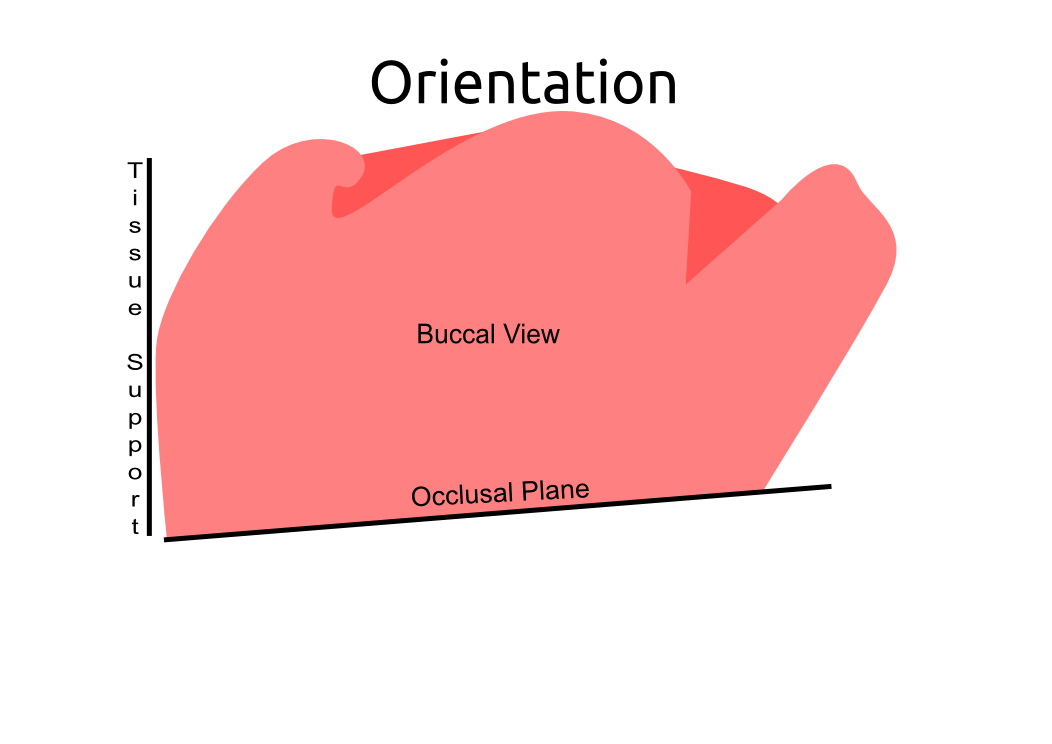
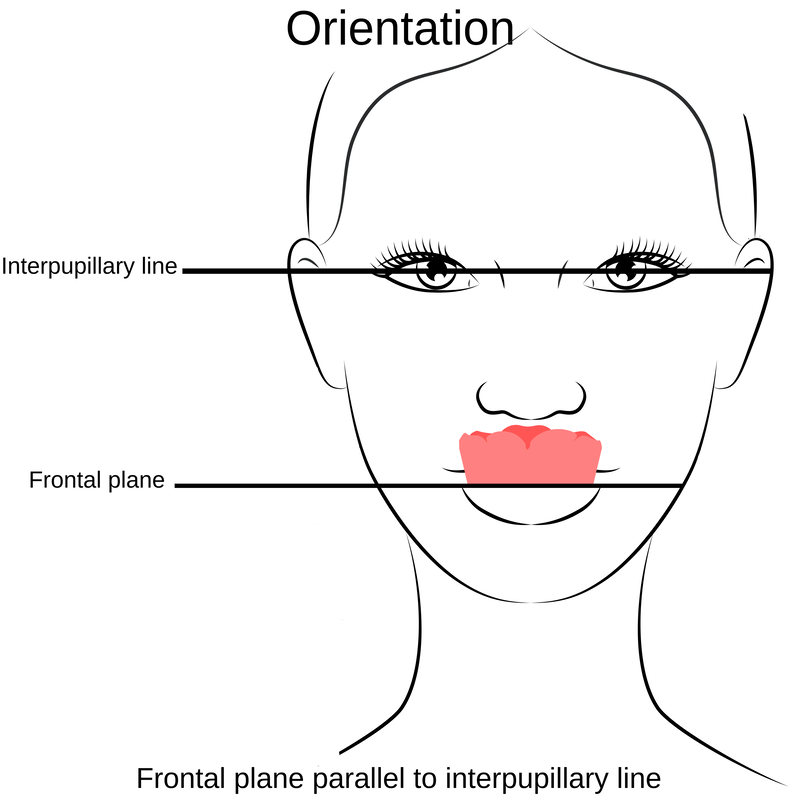
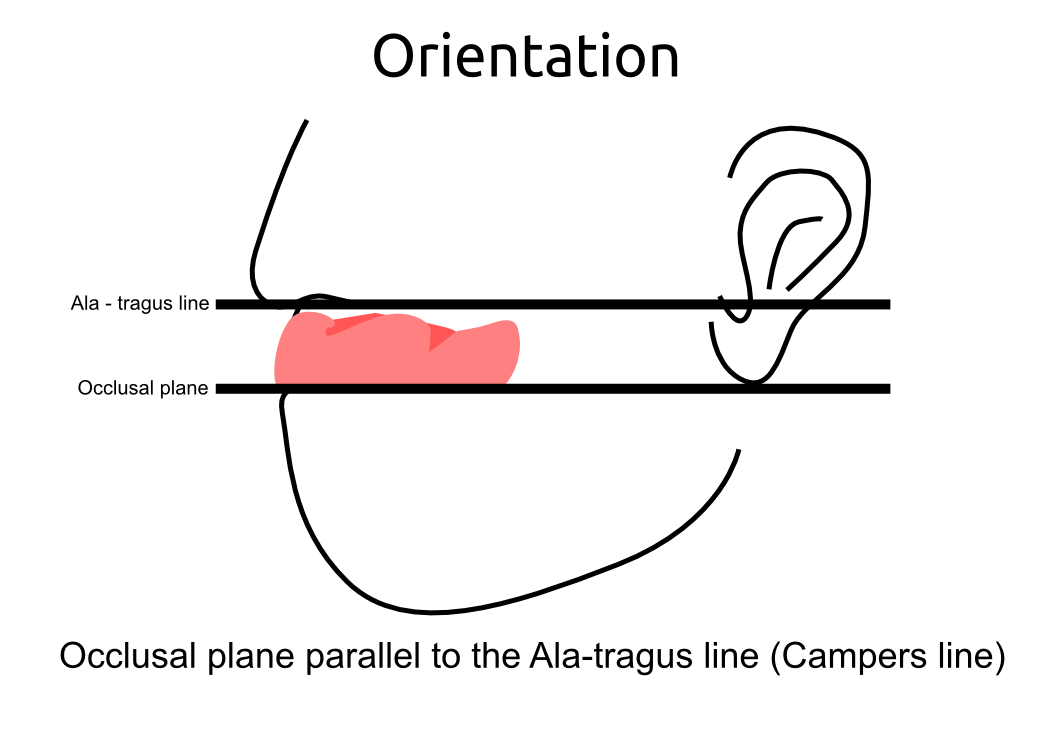
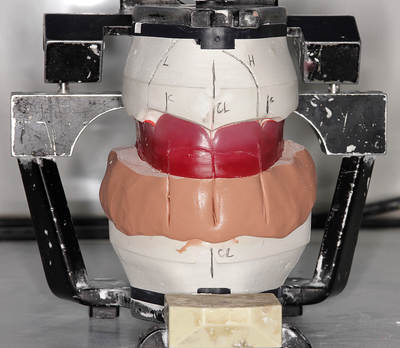
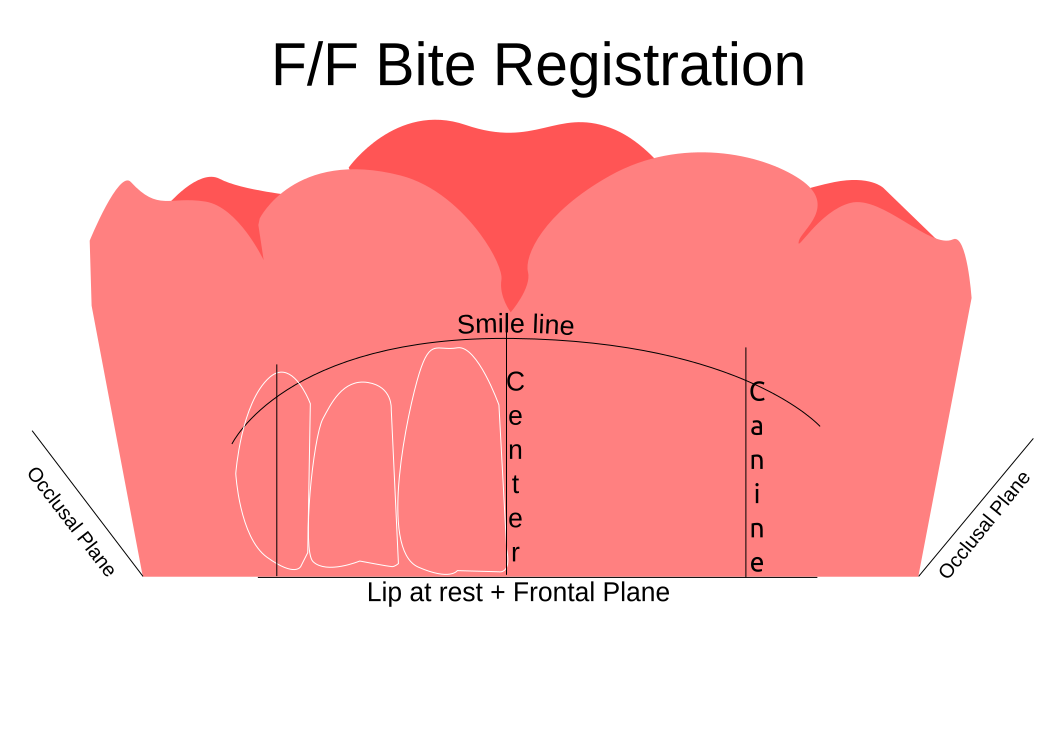
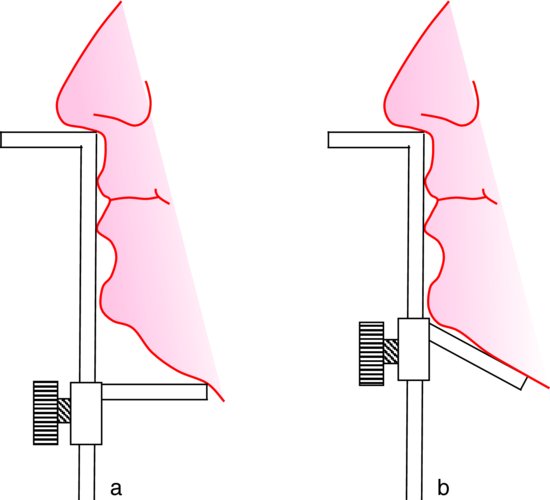
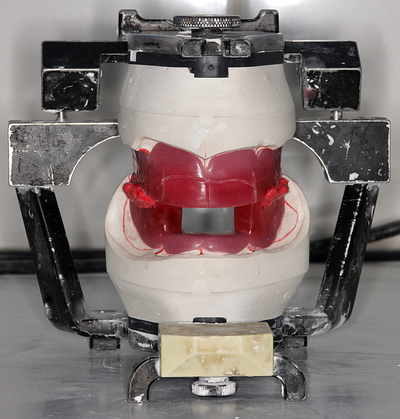
Information from the patients orientation, jaw relationship, OVD, facial & smile features creates the parameters for the dental technician to work within, as the technician will not see the patient, we have to provide this information in a form that they will understand e.g lines scribed on a bite rim or adjusting the bite rim. The retention, extension, stability and support of each base plate would be the assessed individually before continuing. If any of the above is not correct preform an imp wash inside of the base plate and have a new model made. If all of the above is sufficient, continue assessment: Step 1: Orientation Orientation: Frontal Plane & Occulsal Plane A Fox’s bite plane tool is used to establish the orientation of the occlusal plane in an anteroposterior direction (Spee curve) and also the frontal plane against the interpupillary line. With the use of a fox’s bite plane, we assess the frontal plane by placing the fox plane on the bite block anteriorly and checking if it's parallel to the interpupillary line. Adjust the anterior section, if one side is higher or lower until this is level and parallel to the interpupillary line. Use a heated Rim Former or carve the wax. The occlusal plane is assessed by placing the fox plane in the same position and placing a horizontal device e.g ruler from the ala of the nose to the tragus of the ear and making sure the orientation of the fo’x bite plane is parallel to to this. This will set the parameters of how the anterior and posterior teeth will be placed for aesthetics, phonetics, comfort, chewing efficiency and balanced occlusion. Tissue support is determine by preference, clinical decision e.g checking the profile buccally of the previous denture. This determines how far the anterior teeth will be positioned forward and how thick the anterior flange will be.
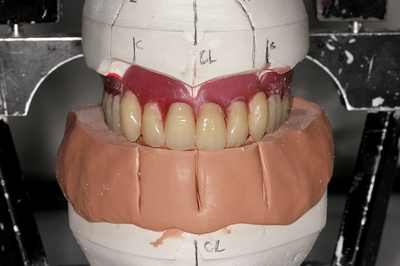
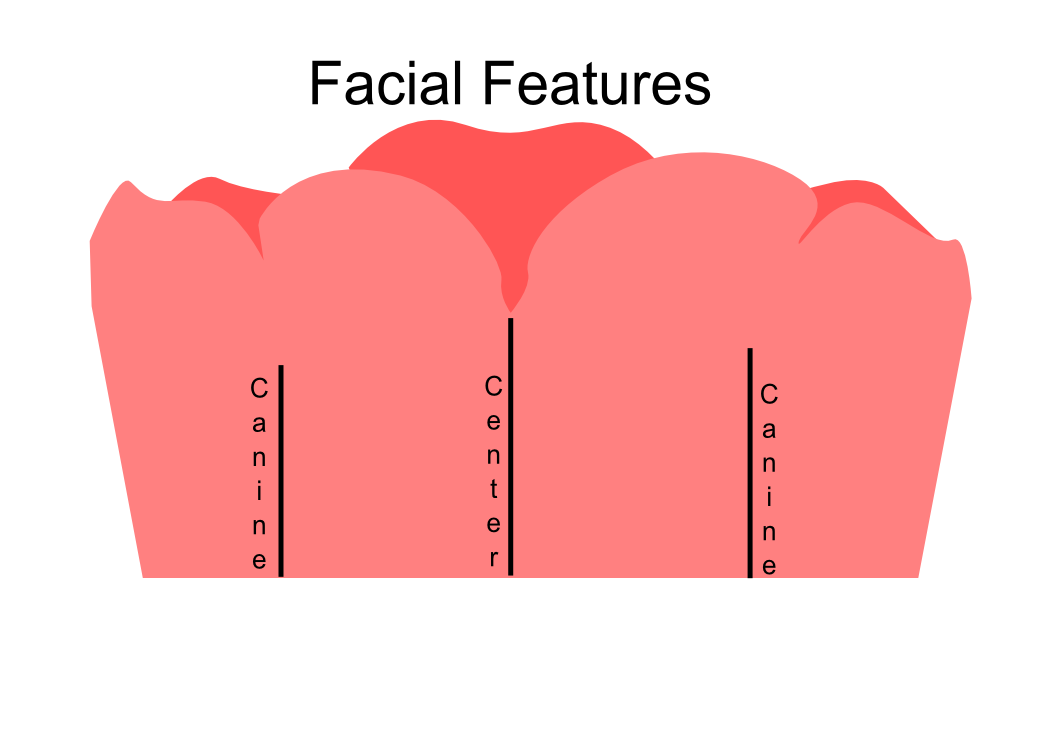
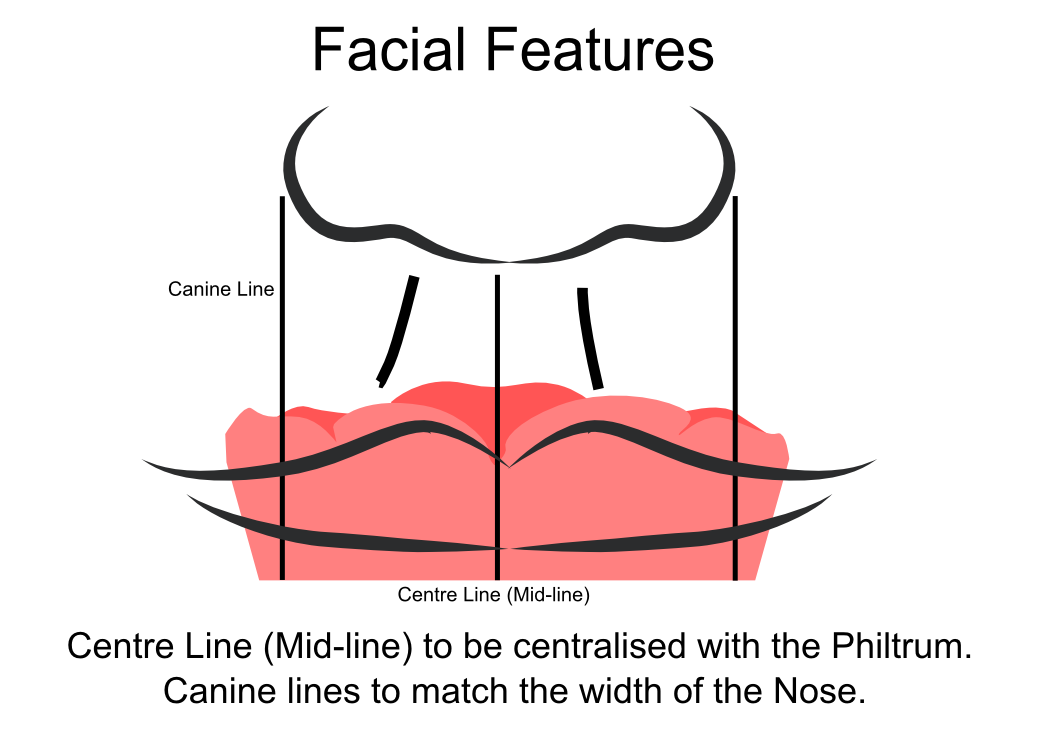
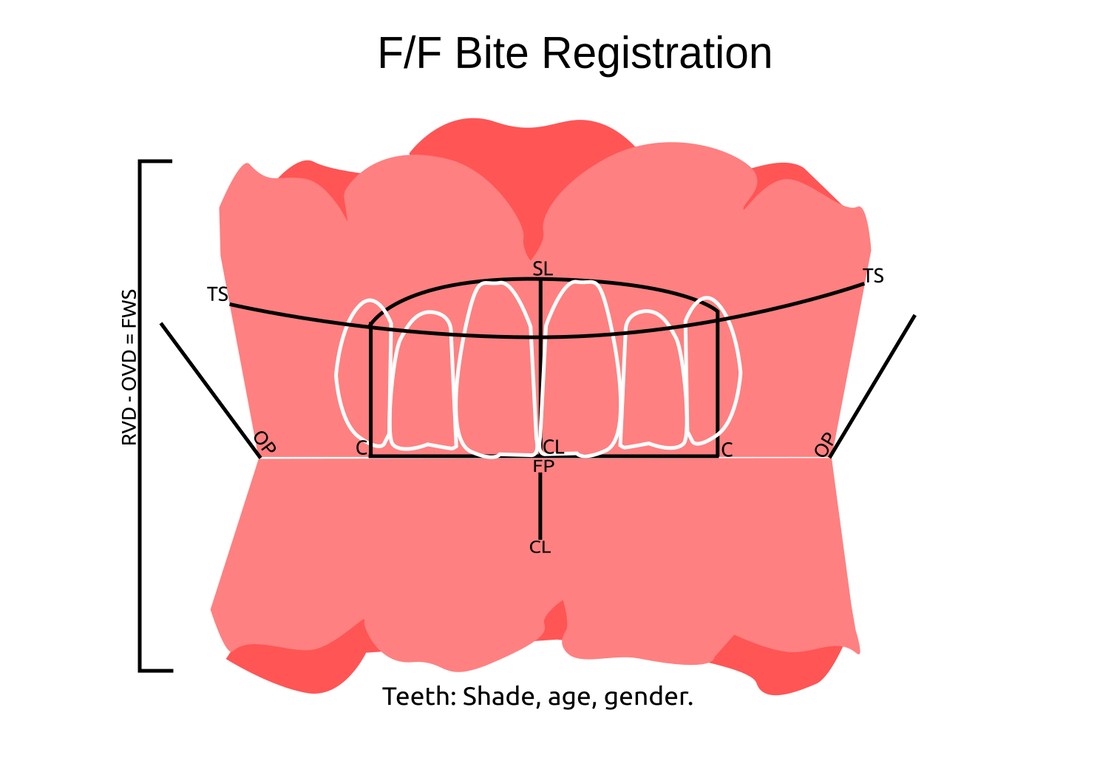
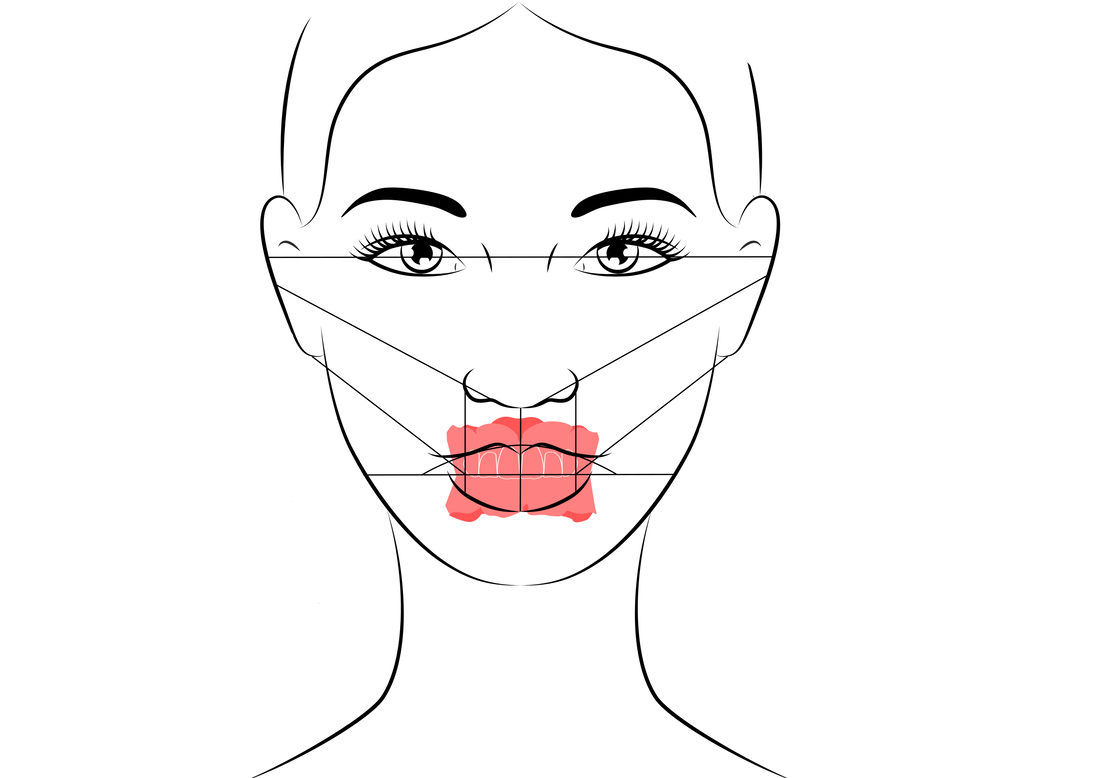
Step 2: Facial & Smile Features Facial Features Facial features sets the aesthetic parameters for the anterior teeth in terms of mould size, shape and selection, e.g width and height of anterior teeth & positioning of the teeth within the centre line & canine lines. All facial features should be scribed onto the upper bite registration with a cold wax knife, DO NOT use a hot wax knife as you can injure the patient. Centre line: The centre line (mid line) is dictated via the philtrum, DO NOT use the nose, as this can give a false reading, as the nose is not usually centralised with the mid line of the face, and can be skewed. This allows for centralisation of the upper centrals to the exact mid-line of the patient. Canine line: The canine lines are dictated via the width of the nose, this is common in 95% of humans. This determines the width of the anterior teeth in relation to the patient. The canines, should not go past this line, unless other factors dictate the canine lines e.g patient preference. The body / labial mesial body should be on or just after this line in the tooth set up, this will allow a natural alignment within the patients facial features.
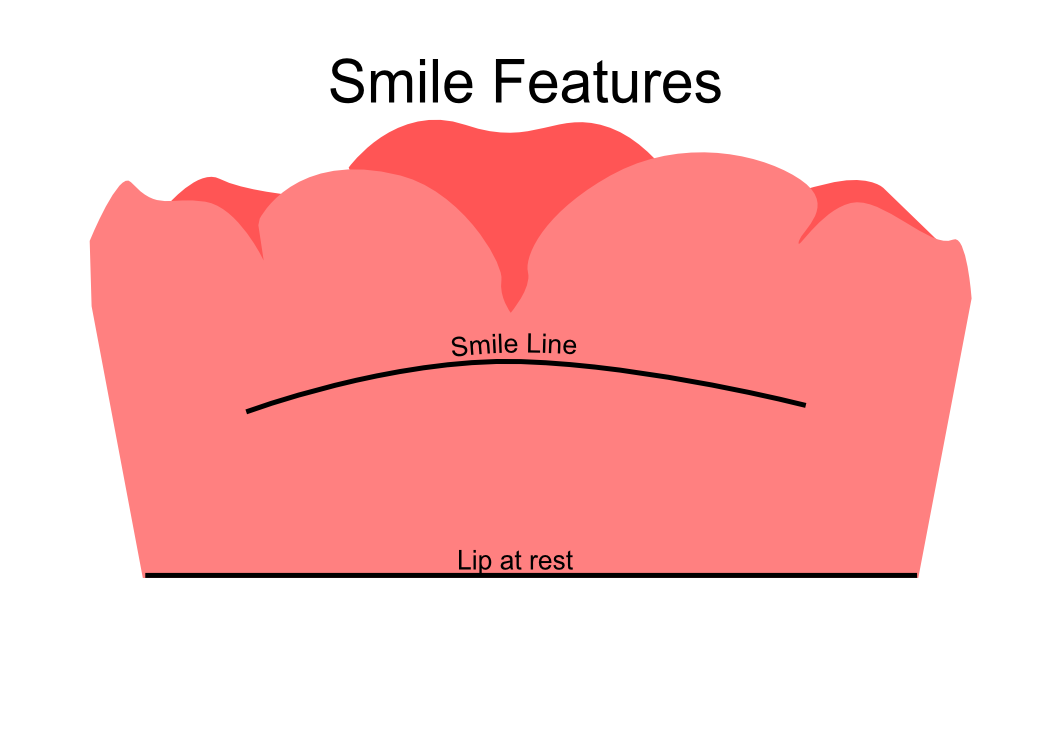
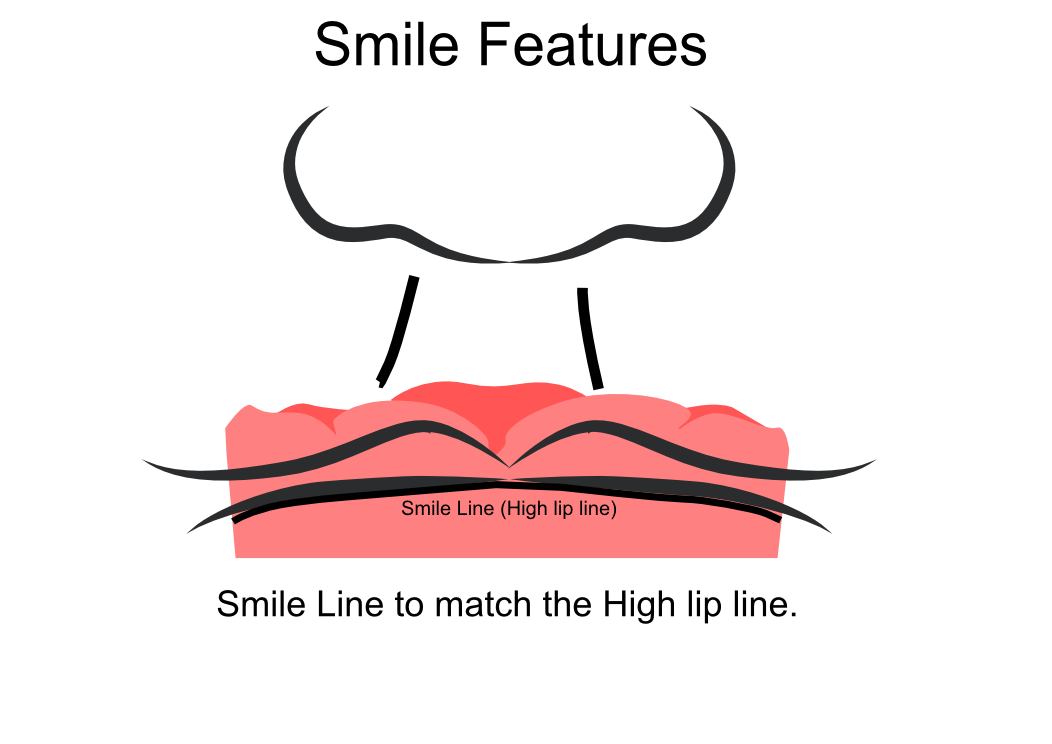
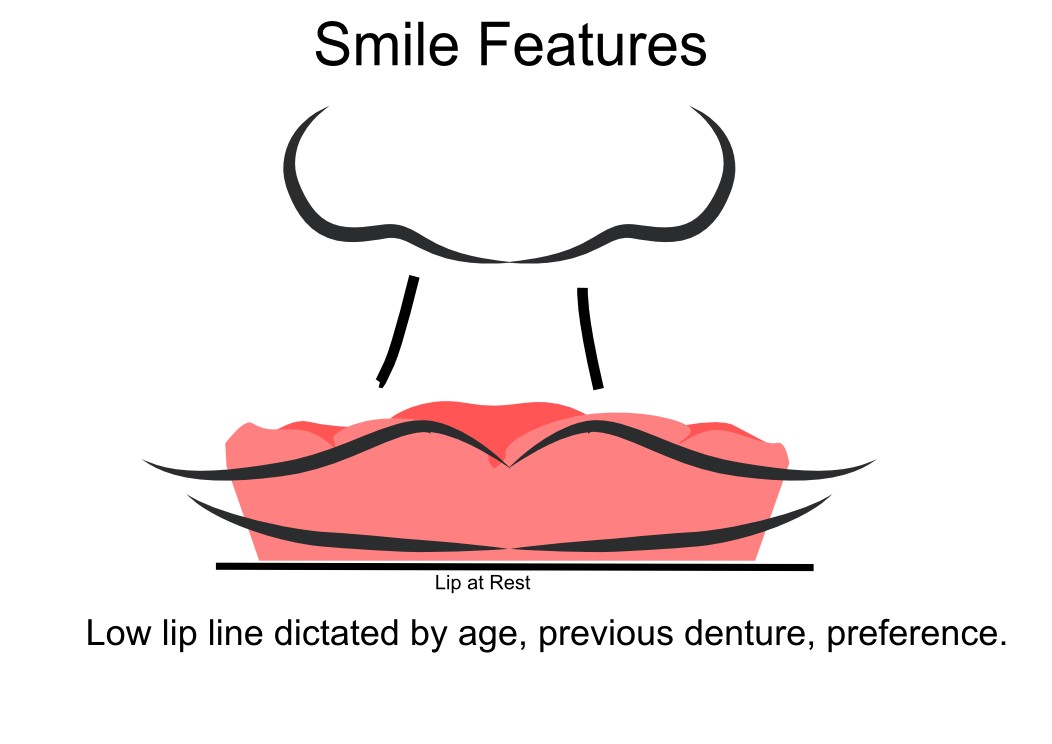
Smile Features The smile features work in sync with the facial features, for the creation of the anterior aesthetic parameters. This also determines how much tooth should be shown when the patients is smiling or how much is shown when the patients lip is at rest. For example when the patient smiles and shows too much gum, this would mean that the smile line should be set higher and the anterior teeth should either be set higher or more of the necks of the teeth exposed to correct the 'Gummy Look'. You can also place a longer tooth if it stays within the parameters of the facial feautres. Smile line (High lip line): The smile line is dictated from the bottom of the upper lip at the highest point (high lip line). Ask the patient to preform a big smile and scribe this on the bite block at that level (cold wax knife, never use a heated instrument). This dictates how much tooth and gum is shown when the patient smiles, it also dictates the dentogenics of the smile by optimising tooth positioning. Low lip line: The low lip line is dictated by many factors including age. Ask the patient or use the previous denture to dictate how much bite rim should be shown and make sure you tell the patient that this is how much tooth will be shown when the lip is relaxed. With the combined parameters of the facial features and smile features, it creates a box, within that box is the parameters for the aesthetics of the denture which dictates, the positioning, width and height of the anterior teeth.
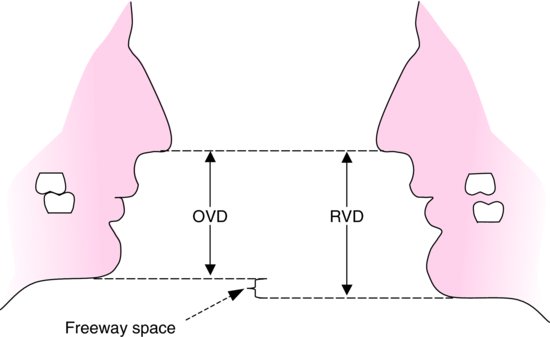
Step 3: Register The Bite OVD, RVD & Free way space Once the aesthetic parameters is set, we need to establish the functional parameters of the bite registration via vertical dimensions, jaw relationship and registering this by locking this information together. The vertical dimension is obtained with the help of a Willis Guage. A Willis Gauge is a tool used to measure the vertical dimension in millimeters between the maxilla and mandible. OVD (Occusal vertical dimension: OVD (Occulsal vertical dimension) is an important factor for patients aesthetics and function. A reduced or increased OVD can cause complaints about aesthetics, function (e.g mastication and stabilisation) and may lead to discomfort. OVD indicates the measurement between the occlusal relationship of the maxilla and mandible. For dentate patients, the OVD is established by occluding the maxillary and mandibular teeth together. In edentulous denture patients, this is established by placing bite rims in the maxillary and mandibular ridge and taking measurements , this can also be obtained from the patients previous set of dentures. RVD (Resting vertical dimension): RVD (Resting vertical dimension) indicates the measurement between the maxilla and mandible when the muscles are relaxed e.g not in occulsion, this is obtained by removing the lower denture and asking the patient to close their lips together without occluding. FWS (Freeway space): FWS (Freeway space) Free way space is between the RVD & OVD measurement of the maxilla and mandible when the mandible is in its physiologic rest position. This is usually between 2 – 4 mm. How to use a Willis guage:
We calculate the FWS by subtracting the RVD from the OVD, this is now the free way space. e.g RVD 47mm – OVD 45mm = 2mm FWS. Increasing or decreasing the dimensions is dependent on the situation, for example if they have an old set of dentures you can use this by placing it into the patients mouth and taking a Willis guage reading and match the bite rims to this. Make sure that the wax blocks have even bilateral contact when establishing the bite. If there is no previous denture present, you can visually see the patients facial muscles in determining if the OVD is correct. Often, if the OVD is increased or reduced beyond it physical dimensions the facial muscles will often indicate this by facial tension. Registering the bite rims: Once the OVD is established, ask the patient to bite together several times and scribe a location mark between the posterior regions of upper bite rim and lower posterior part in a closed position, this will establish a reproducible jaw relationship. Asking the patient to roll their tongue backwards can help with creating a reproducible jaw relationship, if the patient has abnormal bite patterns. Take the bite rims out and cut location grooves into posterior regions of the upper and lower bite rims to allow space for the bite registration material to flow into this area and lock together the U/L bite rims, this will register the bite and transfer the patients jaw relationship into the bite rims and will allow the dentist and technician to verify it’s accuracy. Place the U/L bite rims into the mouth and ask the patient to bite together once more to check if the bite is reproducible via the location mark lines after you have cut the location grooves. Once the bite is reproducible and verified, open or place the bite reg paste in the posterior region areas of the location groove areas and ask the patient to close and wait for it to set. WARN the patient, when they open the bite rim will be joined together. Check and verify if needed. Remember, all of the hard work preformed will not work if a shade has not been taken.
Click the 'NEXT PART 2' button to find out how we transfer this information from the bite registration in the laboratory into a tryin stage. Also see:
#denture #bite #registration #dentistry #dental #laboratory #newsletter #dentist #dentallaboratory #dentaltechnician #dentista #odontologia #teeth #health #healthcare #bremadent #london #digitaldentistry #cadcam #implants #prosthetics #dentures #crowns #orthodontics
0 Comments
 Base plates are the areas that is adapted over the alveolar ridges of the maxilla and mandible and allow for either wax bite rims or teeth to be placed on top of the base pllate. Similar to a foundation of building a house. Base plates tend to be made out of wax to save on costs.
 Triple trays was invented and patented by Dr. S Werrin in the 1980’s with the mantra of “Do it better, easier and faster!” Triple trays are referred to as ‘Dual Arch Trays’ and enables the dentist to capture the prepared restorative areas, the opposing arch and occlusal registration in one procedure. This saves chair time and impression material.
In theory this works, but why is it over 70% remakes in crown & bridge occur from the use of triple trays? Here is some research into this. 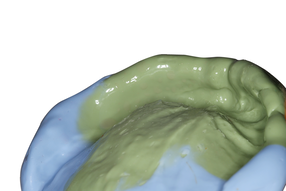 Impressions are key information between Dentist and Dental Labs across the world to transfer reproducible information of the patients mouth since the mid 1800’s. In my time I have found the clinical and technical work is usually of a high standard but why do we have remakes? It’s usually the impression itself.
As a commercial dental laboratory we see 1000’s of impressions weekly. We can only see the physical factors of the impression not the representation of the true I/O information as we do not have access to the I/O of the patient so we cannot judge if the impression is true or false. |
Private Dental Laboratory in London
 Kash Qureshi - Managing Director, Clinical Dental Technician Kash Qureshi - Managing Director, Clinical Dental Technician
About the author:
Kash Qureshi is a Clinical Dental Technician (Denturist) in the U.K who oversees and quality controls over 3000+ fixed and removable prosthesis including implant cases from a clinical and technical aspect monthly at Bremadent Dental Laboratory & Swissedent Denture Clinic in London. www.swissedent.co.uk www.bremadent.co.uk [email protected] 
Categories
All
Archives
May 2024
|





 RSS Feed
RSS Feed