
|
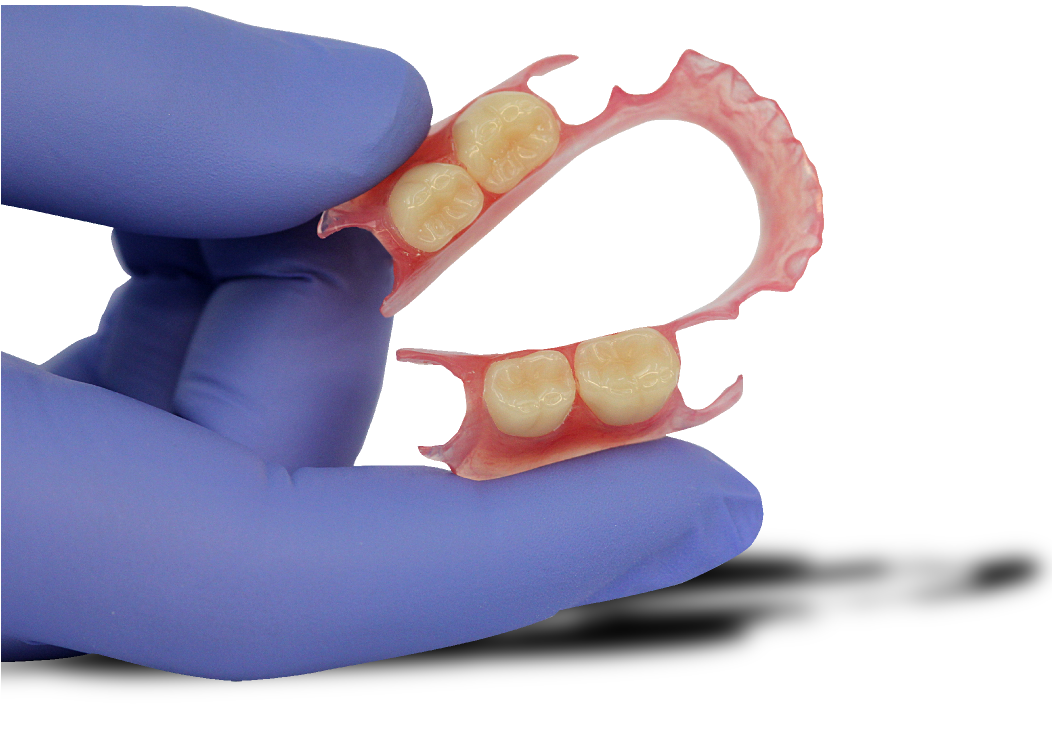
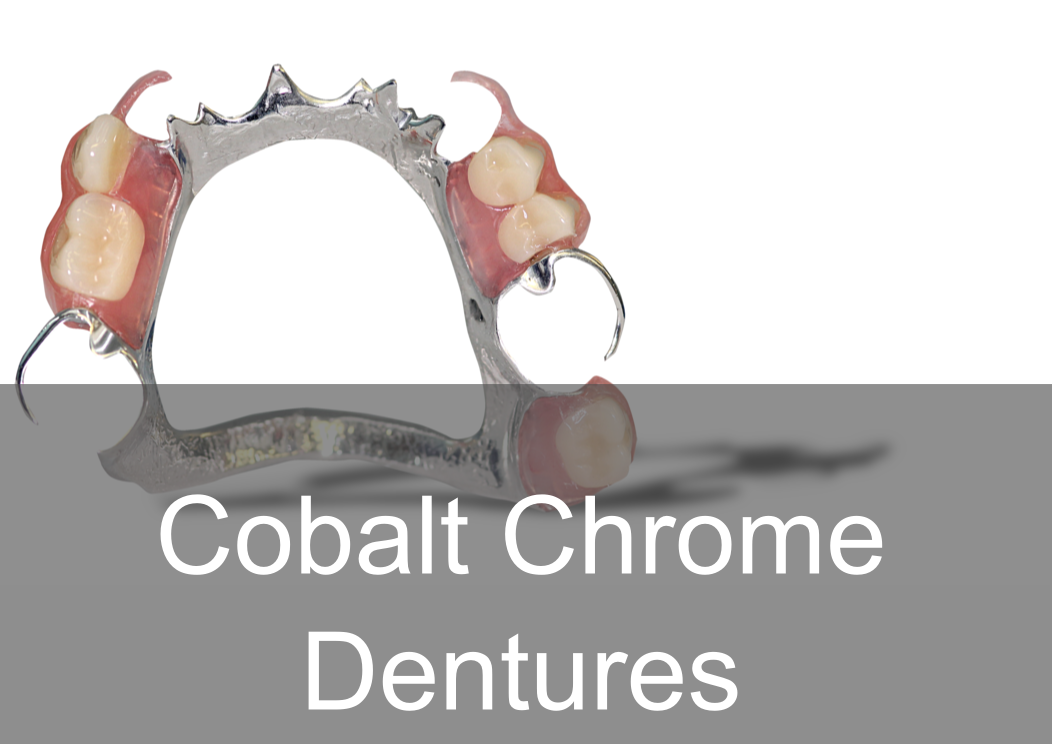
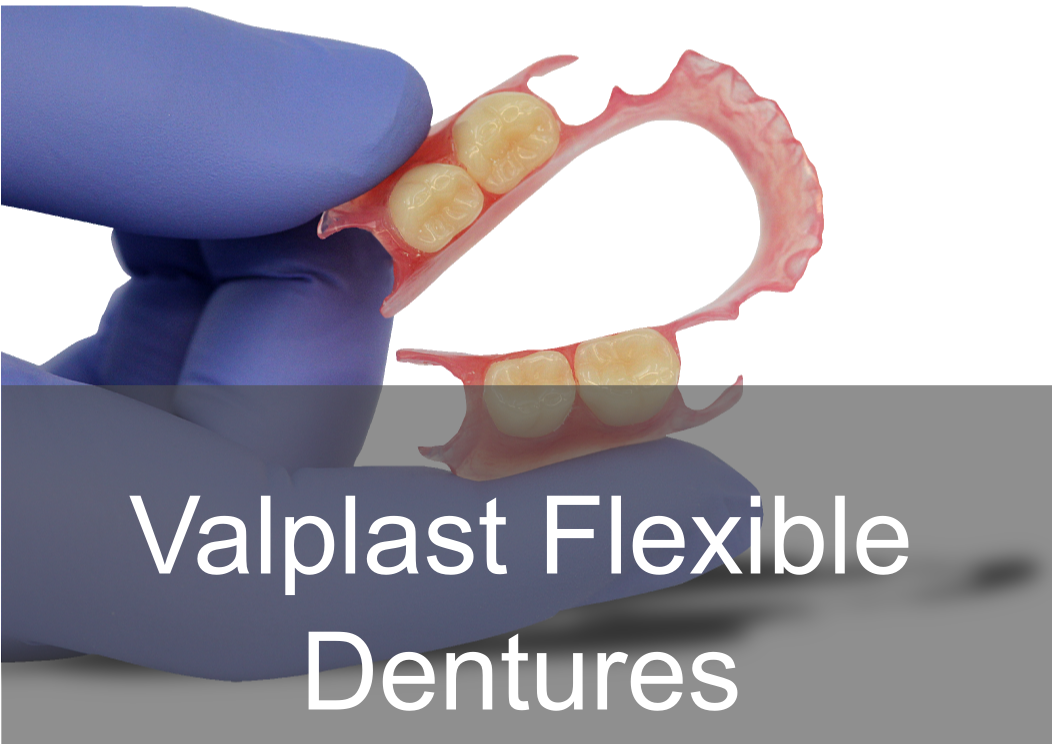
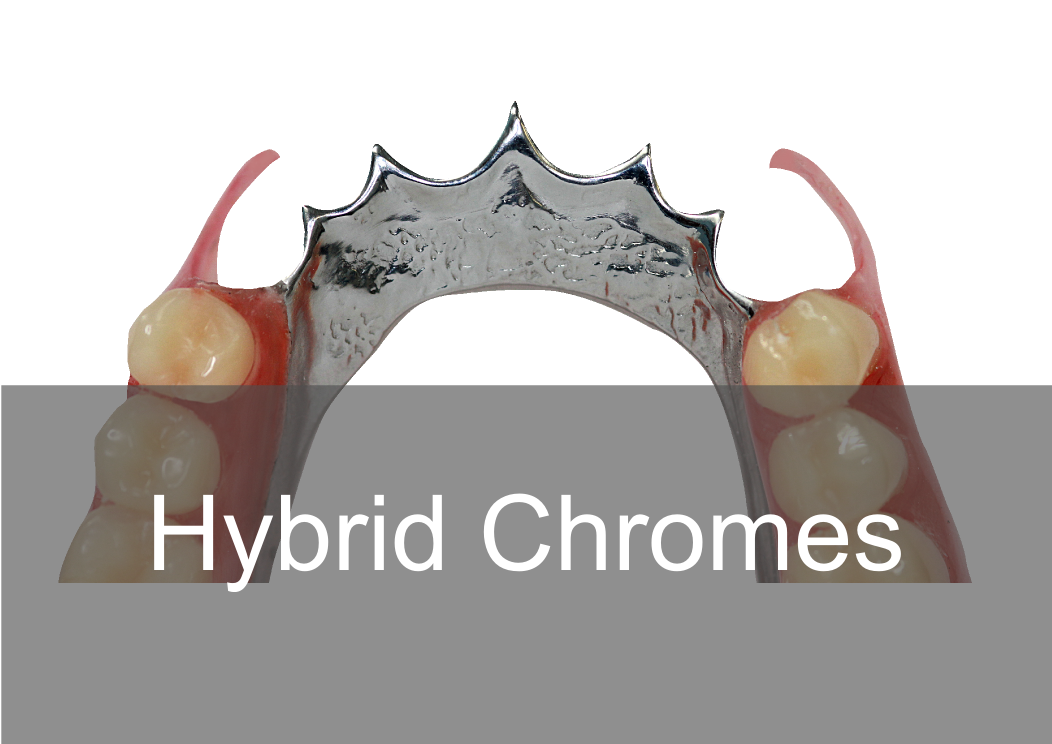
Acrylic, Co/Cr & Valplast RPD Design principles Removable partial dentures assist with mastication (chewing food), help maintain phonetics (speech) and help with aesthetically pleasing to blend in naturally when are teeth missing. They can also help with maintaining oral health and the prevention of over eruption, titling and drifting of adjacent teeth into areas where teeth are missing. They should be designed and constructed to minimise oral damage and is used with a high level of oral hygiene from the patient. The underlying principles of support, retention and stability should be understood whatever type of partial denture is to be made. With any form of dental treatment the main aim is to provide dental treatment than provides function and aesthetics that manages the patients expectations within the limitations. Treatment plan Before any treatment, there are crucial clinical stages that set the foundation of designing a partial denture. Obtaining the patient history which will indicate the parameters of expectations and I/O, E/O examinations that will indicate the limitations. You will then be able to formulate a treatment plan that will manage the patient expectations within the limitations. Within the treatment it’s a good time to find if they are allergic to anything e.g latex, nickel, monomer etc. The natural teeth should be examined, their number, position and occlusal relations noted, and evidence of caries, plaque, periodontal diseases and tooth mobility recorded. The state of the mucosa should be examined and previous dentures inspected in relation to the natural teeth and the patient’s experience. Radiographs of the teeth and supporting tissues may be necessary. Pathological conditions should be investigated and treated appropriately. Extraction of teeth, periodontal treatment or restorative treatment of any kind should be completed prior to partial denture construction. However, it is essential that the provisional design of the dentures is made early in the treatment plan so that the most appropriate restorations are placed in any natural teeth which will act as abutments for the partial denture. When crowns or cast restorations are to used to restore abutment teeth they should be designed to incorporate suitable features for the partial denture (e.g. guide planes, rest seats, milled ledges and suitable undercuts for clasps). Dietary advice and attention to oral hygiene should be given as appropriate. Design principles for RPDS : There are various resources online with information that go into detail on RPD’s. This guide simplifies the design principles with the key components that a dentist and dental laboratory will need to create a successful RPD. After any clinical assessment, primary imps should be taken to assess the design of an RPD: Main stages in design principles of any RPD: Step 1: Patient expectations, parameters, limitations and future proofing Step 2: Surveying and design of RPD within expectations, parameters and limitations Step 4: Mouth preparation, rest seats, guide planes and retentive areas Step 5: Construction of RPD within surveying, design, expectations, parameters and limitation Most common types of removable partial dentures: Acrylic (Plastic) Cobalt Chrome (Co/ Cr, metal with acrylic saddle areas) Valplast Flexible (Nylon flexible material) Minimum thickness RPD’s (mm): Acrylic: between 3 – 4 mm Cobalt chrome: - between 1 – 2mm (can go beyond it’s limitation) Valplast: 1.5mm You can go beyond this minimum thickness within reason, but risk weakening the materials mechanical properties and may cause it to break. How do you choose what material is best for RPD’s ? There are many factors that influence this decision:
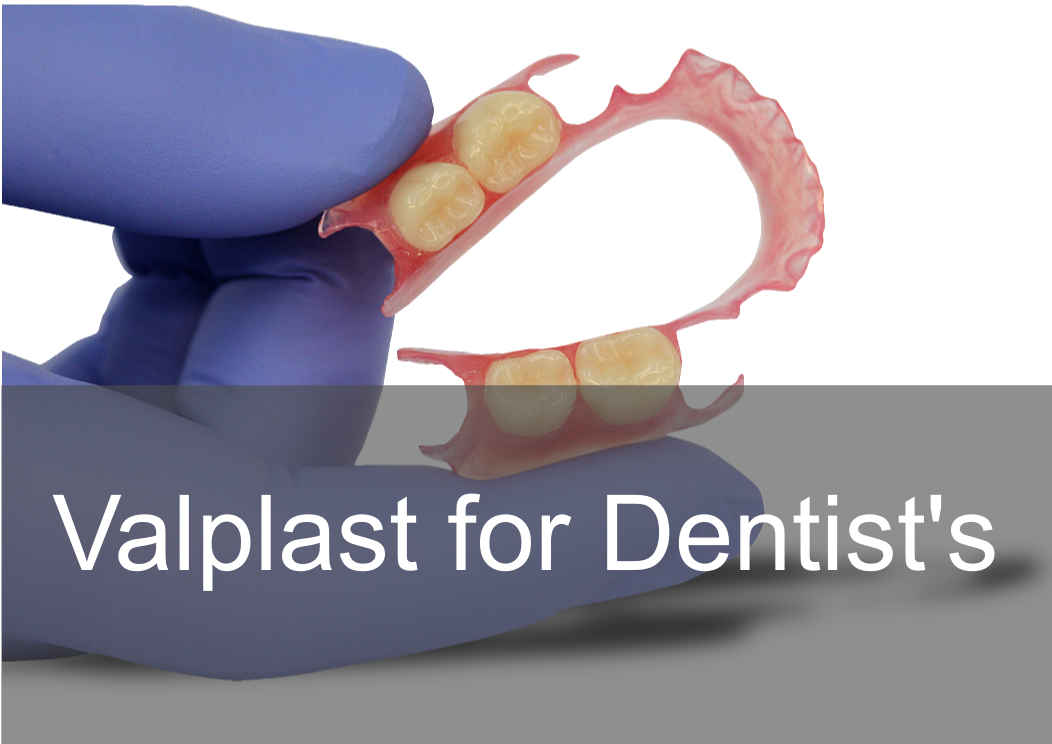
After primary imps stages: After taking the primary impression ask the laboratory to cast study models and design a RPD based on the patient expectation and parameters. When you have study models to hand, it allows you to see everything from all angles and will help with the design process. It allows you to evaluate the occlusion, adjacent teeth, connector design, retention and support areas and surveying a path of insertion. The design will also highlight areas that may need preparation within the mouth e.g there may be no space for a rest seat as the occlusion is too tight as shown on the articulated models. The main areas of preparation in the mouth are rest seats, guide planes and retentive areas. The study model, design on the model and a secondary special tray impression should be sent for the next stages for rpd construction. A secondary impression is required for more accuracy, a primary impression is more a diagnostic tool. Please see below a Co/Cr RPD design sheet to download in.pdf and print and send with your case! 5 Components of any RPD :
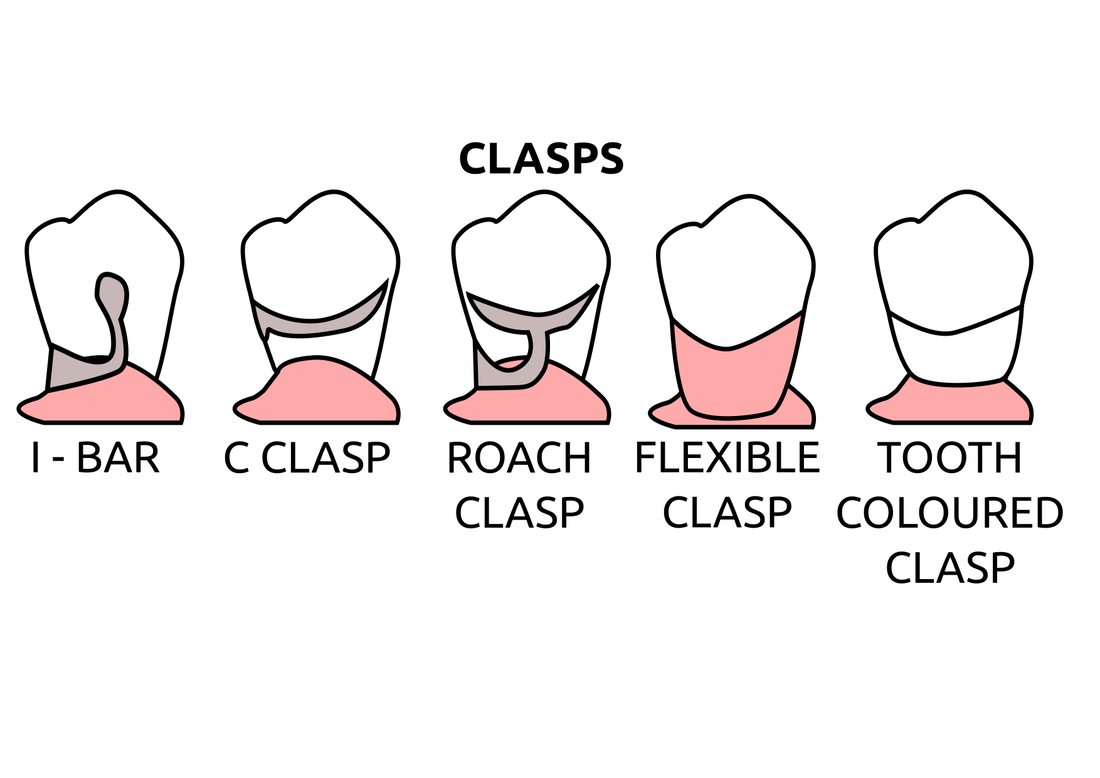
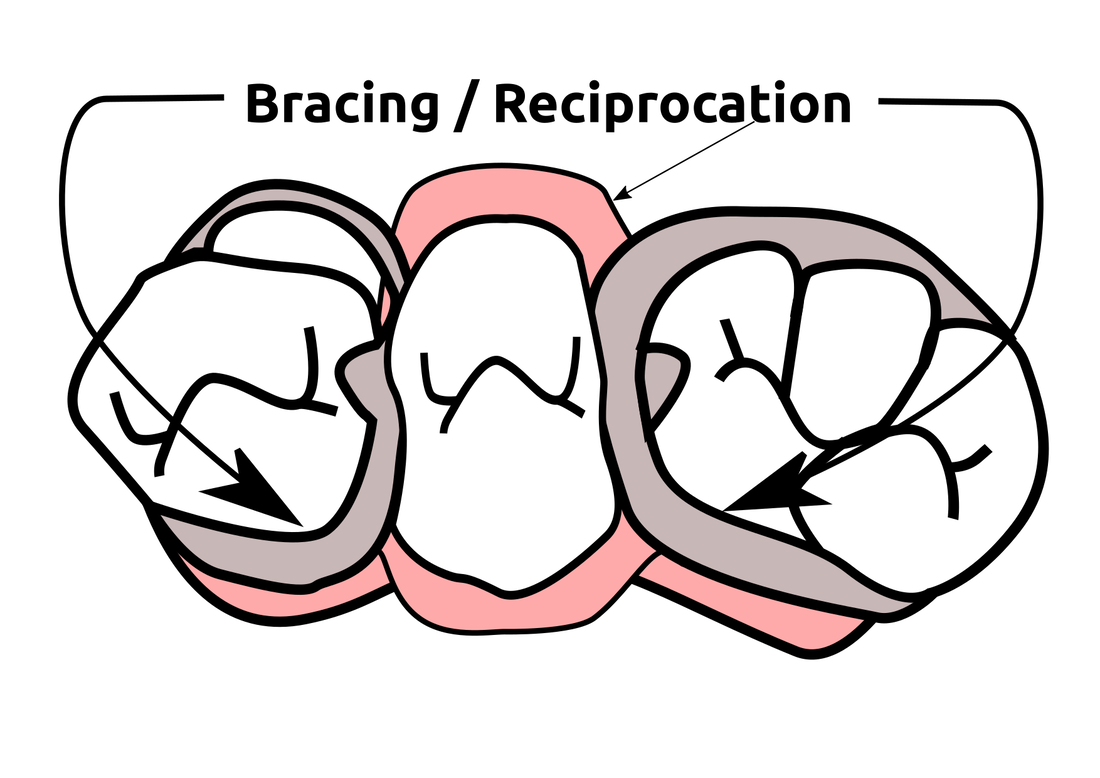
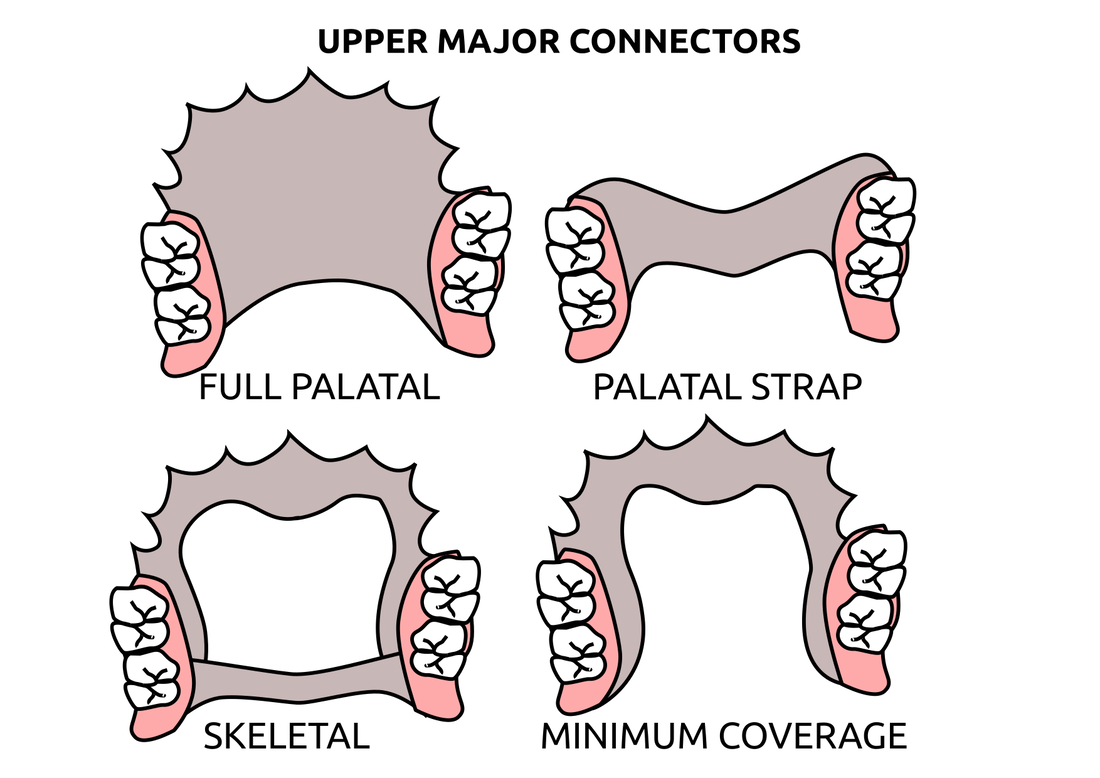
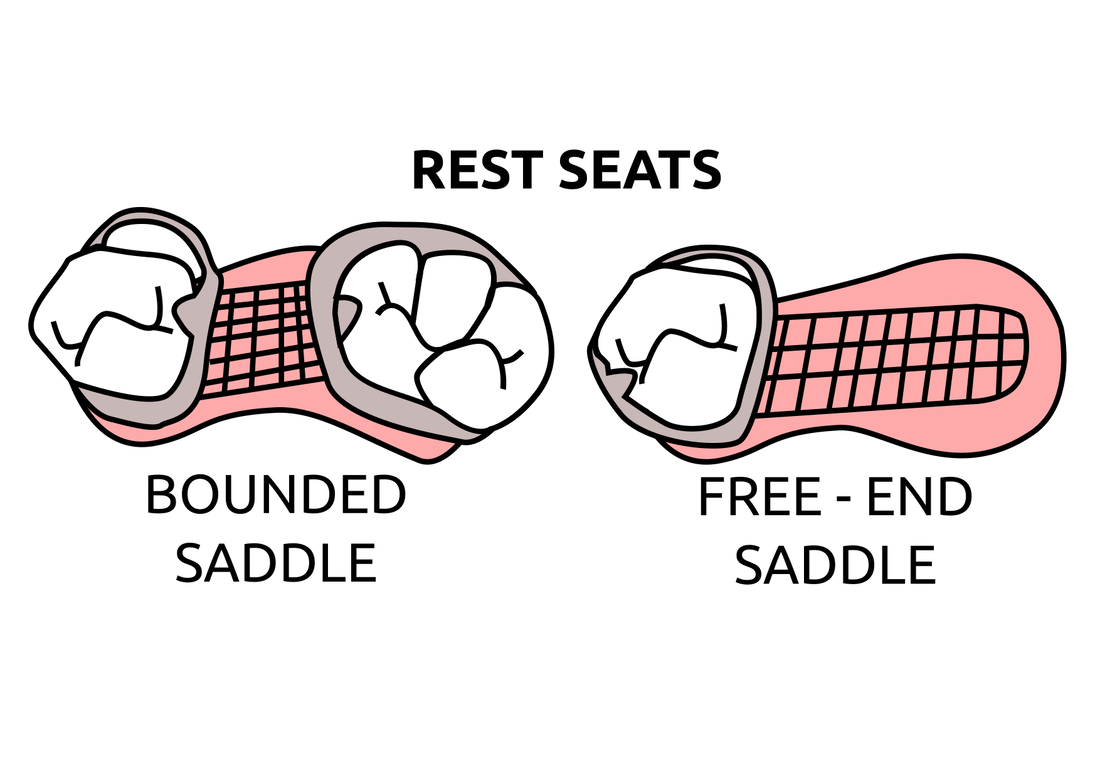
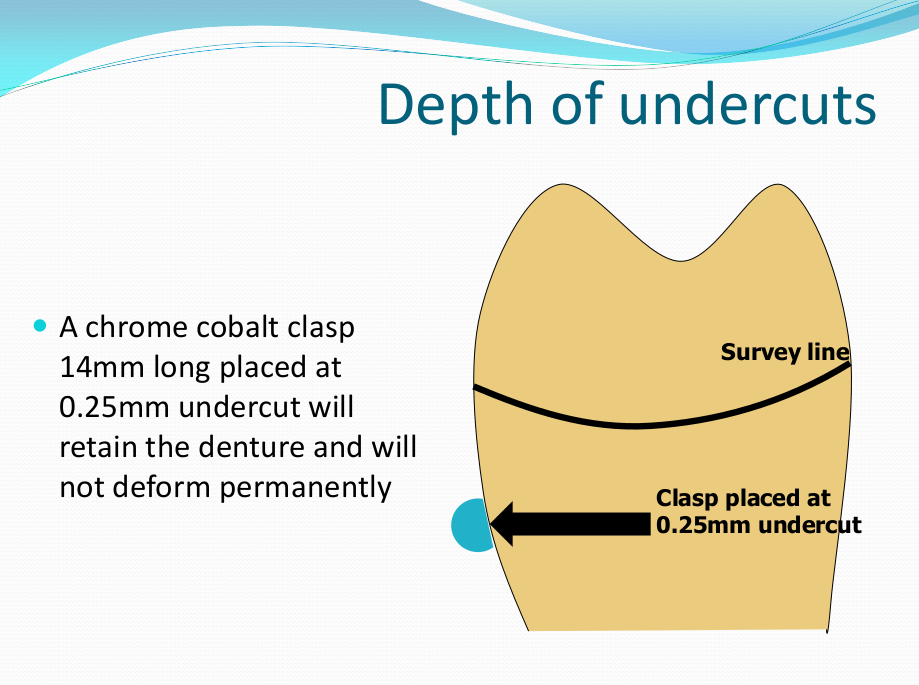
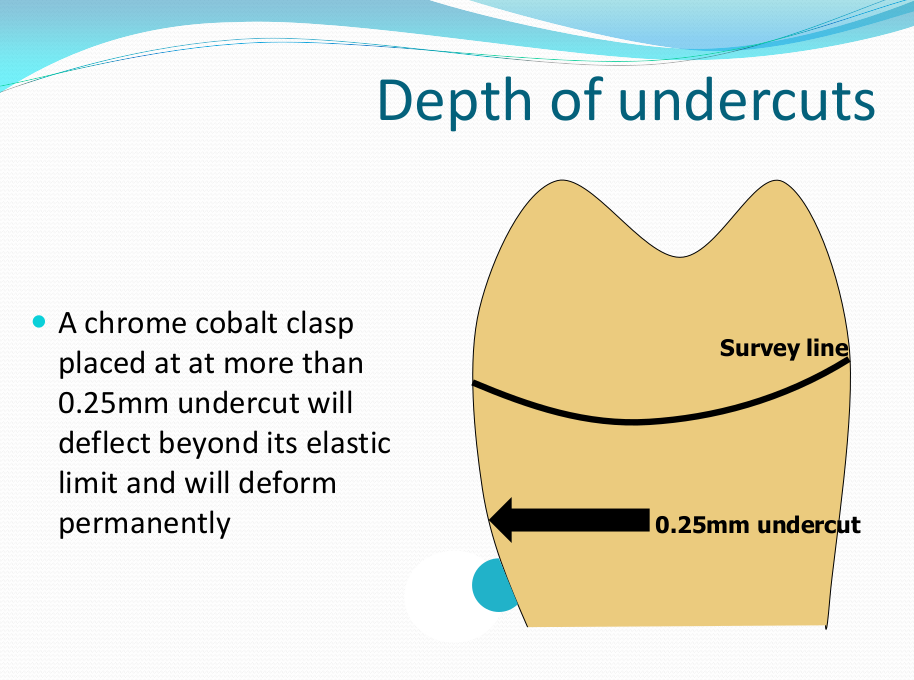
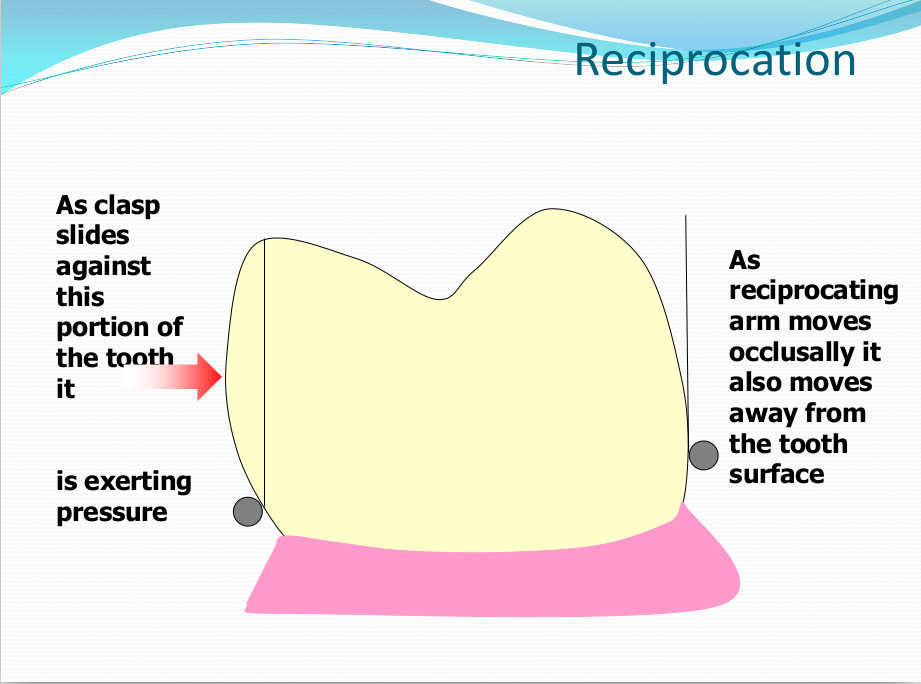
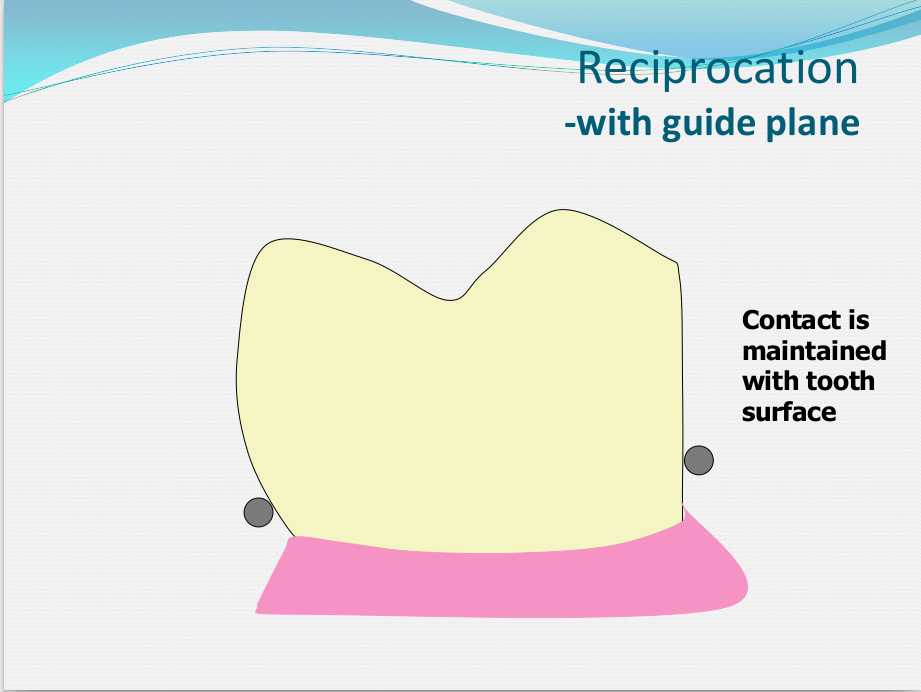
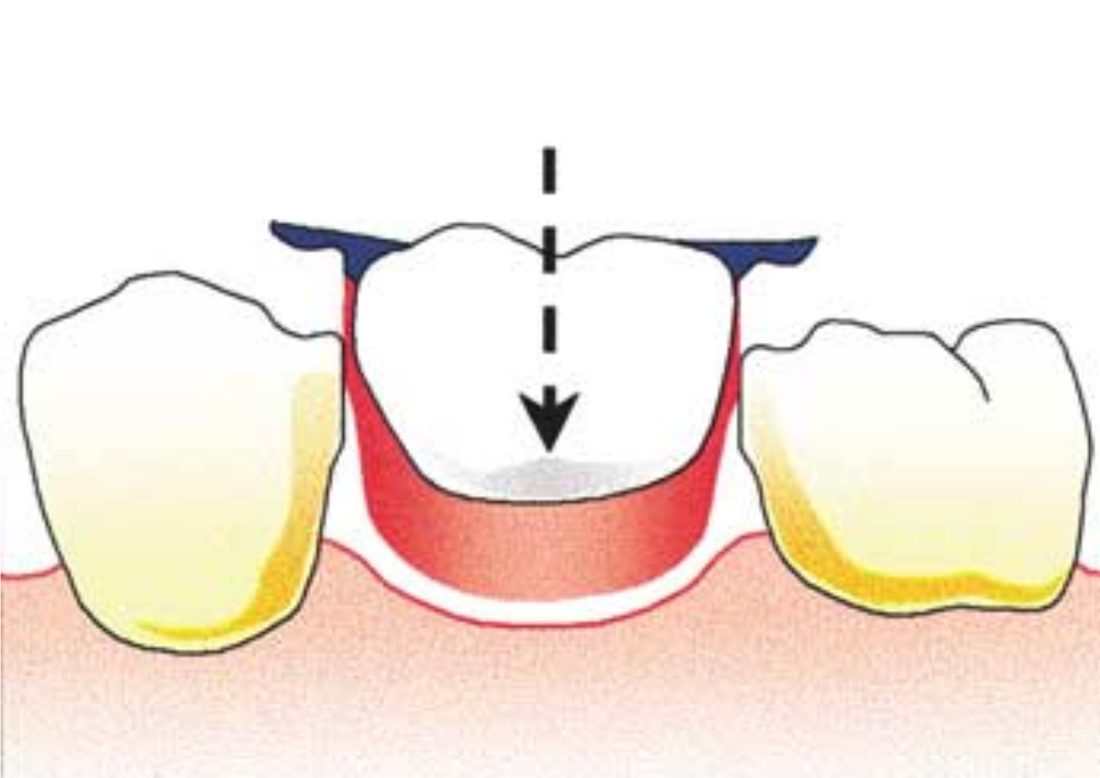
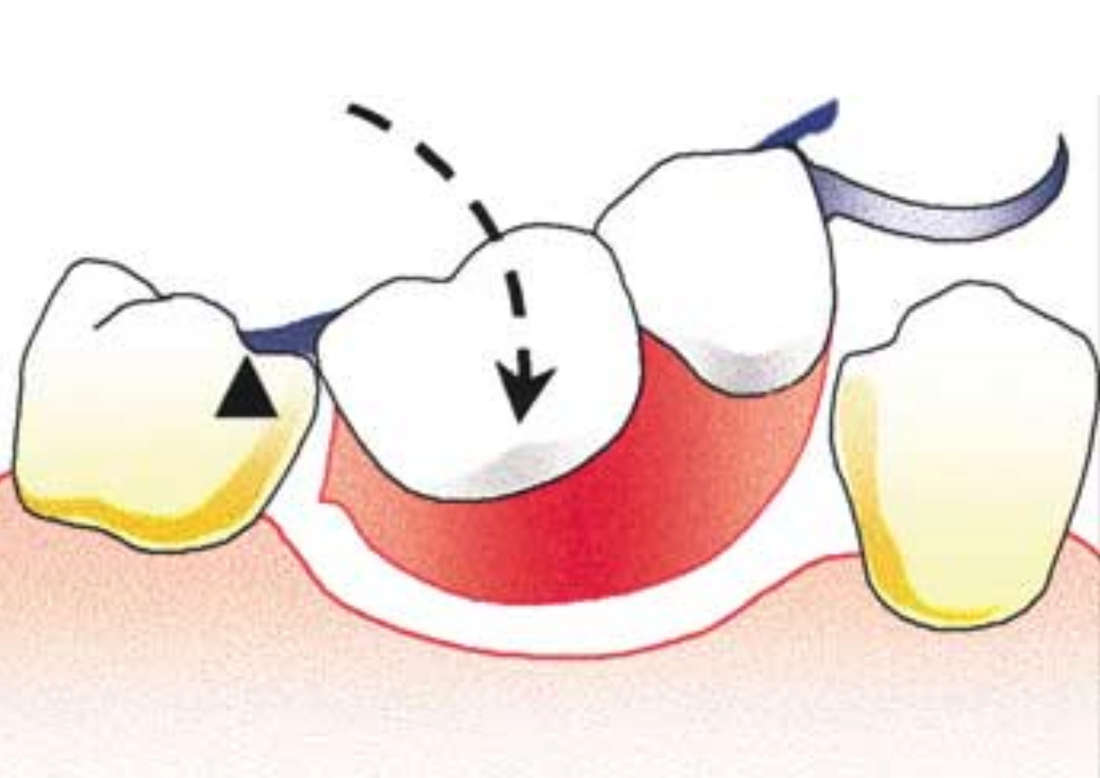
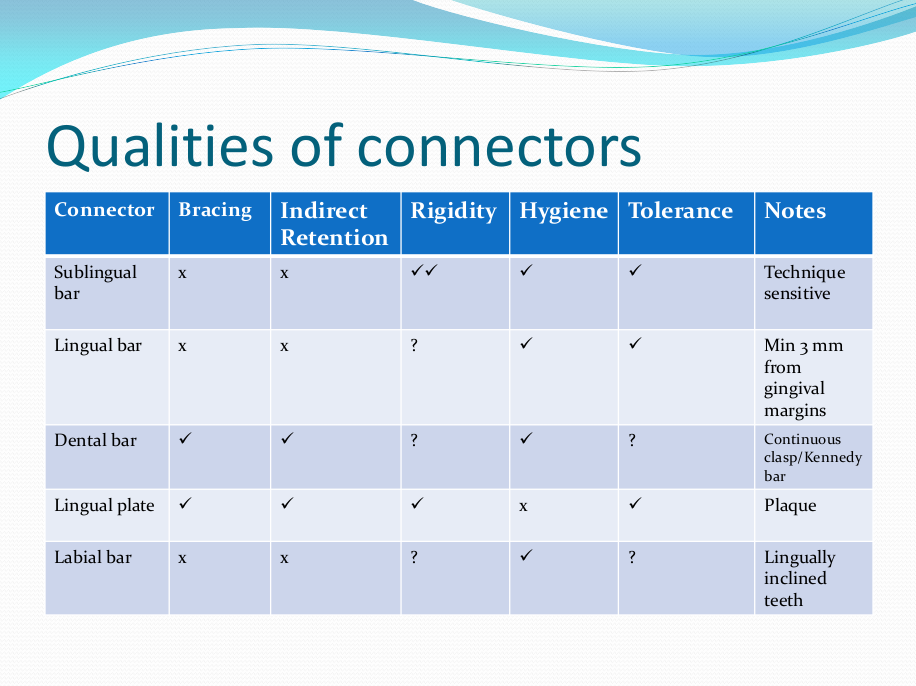
Saddle: The component or components that provide the area of where the teeth are placed and provide the flange extensions in acrylic of an RPD. Support : The function of a component or components to provide resistance to displacement towards the oral tissues on function. Force is transmitted to: Mucosa via palatal areas, saddle areas. Teeth via rest seats, occulsal, cingulum, incsical. Retention: The function of a component or components to provide resistance to displacement away from the oral tissues on function via: Mucosa coverage: Giving aheshion / cohesion NB Muscular effort: Tongue, Cheeks, Lips Clasps – C clasps, roach clasps, I bar Ideal clasps: For clasps to be effective, the tips of the clasps must be engaged into an undercut with an ideal depth of undercut at 0.25mm. For a chrome clasp the ideal minimum length is 14mm For a wrought stainless steel clasp a minimum of 7mm. Studies have shown anything below the minimum length are subjected to deformation and became non retentive. If a clasp is placed at more than 0.25mm of an undercut it will deflect beyond it’s elastic limit and will deform permanently. Depth of undercuts Deep undercut do provide more retention but co/cr clasps that engaged into a deeper undercut have to be more flexible to prevent permanent deformation. Stainless steel wrought clasps are more flexible and is favoured in this situation. If there is undercuts, e.g due to short teeth or conical teeth, it’s possible to create an undercut by the use of composite bonded or trim the teeth to create an undercut. Indirect Retention Rest seats on the RPI system on a free end saddle will have the rest seat on the mesial aspect of the tooth. On a bounded saddle it’s common to place the rest seat next to the saddle area. A study has shown retainer designs with distal rest seats tend to move the clinical crown distally and the root mesially at the apex, resulting in horizontal forces in the bone. By placing rest seats more anteriorly provides an axis of rotation that directs applied forces in a more vertical direction. What is the RPI system in Co/Cr ? It’s short for rest, plate and I bar clasp. The rest seat is placed on the mesial aspect of the tooth with an I bar clasp placed on the tooth and retention mesh for acrylic. Bracing and reciprocation The function of a component or components to provide resistance to lateral displacement during function via extension of flanges into the full depth of the sulcus and the reciprocal arms and non retentive components of clasps. What are guide planes? They are prepped areas on teeth adjacent to an edentoulous area and assist with bracing and reciprocation and path of insertion. Path of insertion: This is obtained by placing the models onto a surveyor and assessing an ideal path of insertion and displacement whilst highlighting the ideal depth of undercuts for retention. This is a vital tool and uses a graphite rod and various tools to block out and keep undercuts for a path of insertion. There are many types of paths of insertion for RPDS, we have three main categories, single, multiple and rotational which is determined by the tooth undercuts, infrabulge & suprabulge, guide planes, tissues and anatomy. Connector The connector design is based on many factors from patient expectations and preference, parameters, limitations and future proofing. Wherever possible, connectors in chrome’s should be placed at least 3mm away from the gingival margins and should be designed with hygiene and the least amount of risk to adjacent teeth in mind. The most common types of connectors are bar and plate. Bar – Feel bulky but are kind to the mucosa. Plate – Covers more of the mucosa palatally and lingually and is less noticeable to the patient Please see below our information on our laboratory services for reemovable prosthetics : Also see guides on:
0 Comments
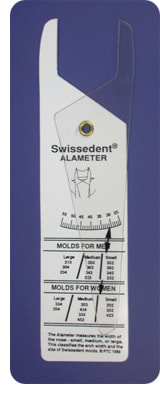
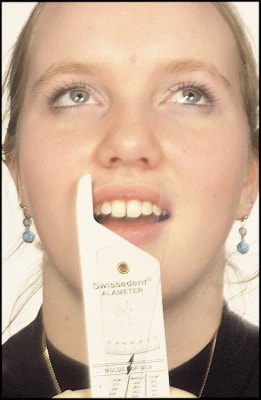
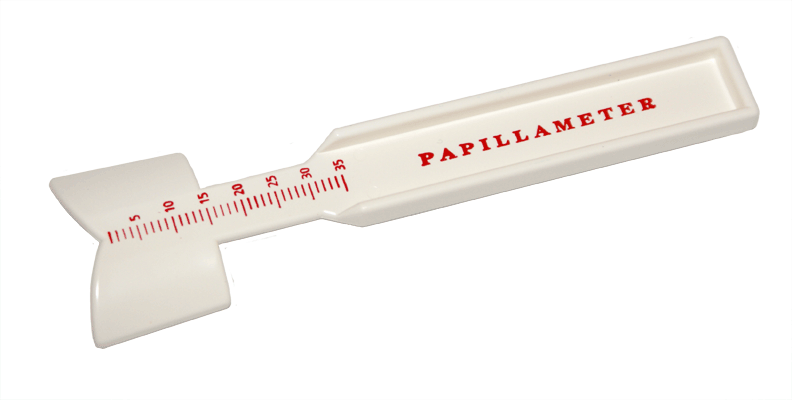
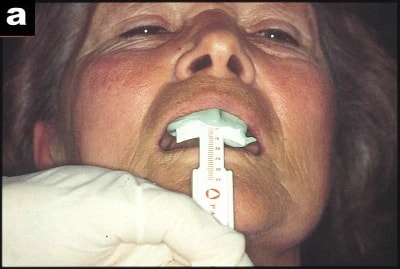
In 1951 Dr. John P. Frush, a graduate of the University of Southern California School of Dentistry, travelled to Switzerland to attend a postgraduate course in complete prosthodontics where he learnt about new procedures and products to restore the natural appearance of edentolous patients. 1 year later Dr. Frush landed exclusive distribution rights from Candulor AG to distribute their Swiss line of denture teeth in North America. Candulor sponsored Dr. Frush on this course and manufactured the most natural looking denture teeth Dr. Frush had ever seen. He then made a deal with Candulor to privatise a line of porcelain teeth under his company, Swissedent called the Swissedent 900 Series. Dr. Frush later developed and patented macroscopic colour changes in the anterior porcelain denture teeth, which occur in natural dentition as a result of progressive incisial wear and pigmental penetration as a result of facial cracks in the enamel of the central incisor teeth which also included the blueish incisal edges of the lateral incisors. This became known as the physiologic colour combination, derived from the study of natural dentition. Dr. Frush was a true visionary and wanted to change the denture industry beyond the sales of Swissedent teeth. He needed to develop the tools to go along with the Swissedent teeth to educate his fellow Dentists so they could also develop a more natural looking denture and gave him ideas of developing a new form of denture occlusion designed for edentulous patients. Dr. Frush spent six years researching and developing, from his clinical research he found most denture wearers suffered with the stability of the lower denture, which was caused by opposing forces, created by the cusp occlusion. Monoplane occlusion was only used by a small number of Dentists due to its lack of bilateral balance and problems with functional mastication. After six years Dr. Frush approached Candulor to produce Centrimatic posterior teeth under the name Swissedent 900 series that had bilateral balancing throughout all function and eliminated all interceptions and inclined planes that created the instabilities. Dr. Frush then formed the Swissedent Foundation an educational part of his company to help fellow dental professionals. He produced a series of six articles for the Journal of Prosthetic Dentistry on the Swissedent Technology between 1956 and 1958. The information in the article became the required reading for Dental students in most Dental schools and gave over 300 courses on Swissedent protocols to graduate dentist and dental technicians, 50+ years later the same principles are at the forefront of most premium denture systems with only the aesthetics changing. In 1960 Dr. Frush developed a device that made the anterior moulds more aesthetically pleasing and unique to the individual called the Alameter (Figure 1,2 - BDJ Nature.com), along side other devices developed called the Papillameter (Figure 3,4 - BDJ Nature.com), Rim Former (Figure 5, 6 Blue Dolphin Products) and Esthetic Control Base. The Alameter was developed from studies that showed 96% of human noses where the same width as the four front anteriors. The Papillameter was developed to determine the distance in length from the incisive papilla to the upper lip at rest, which established how much tooth should be showed when the patient was relaxed. All of the devices developed is used to determine the optimum mould for the patient as well as the natural independent positioning of the anterior teeth according the age, sex and other factors of the patients. In 1987, the Swissedent Corporation was sold to the John Ness of the Productivity Training Corporation (PTC) with conditions that Dr. Frush retained ownership of the Accu-Dent Reasearch & Development.
Mr. Ness was the founder of the Productivity Training Corporation and was well known for his ability to develop techniques that were easily understandable and transferable to other Dental Technicians. In the 1980s Mr. Collin Lee a Qualified Dental Technician who owned one of the biggest and successful Dental Laboratories in the U.K, obtained exclusive rights to distribute the PTC system in the United Kingdom. In the late 1980s a group was formed in the United Kingdom called the Private Prosthetics Group, which consisted of dentist and dental technicians and included Professor J. Fraser McCord, a graduate from Edinburgh University in 1970. Professor J. Fraser McCord provided articles, lectures and courses in the United Kingdom on the Swissedent System for other dentists and dental Technicians. 30+ years on and the articles are still required reading material for creating natural looking dentures. In 1992, PTC had lost the right to sell the Swiss Line of teeth and products in North America from Candulour and also sold the right to use the name Swissedent to Austenal and Dentsply, which labelled Kenson teeth with the Swissedent brand. In 1993, Dr. Smudde realised that this had taken place and knew that action had to be taken to bring the Swissedent brand back, Dr. Smudde went to Switzerland and acquired the distribution rights from Candulor for the same teeth imported and distributed by Dr. Frush under the name Swissedent. In 1994, Dr. Smudde formed Geneva Dental and created the trademark for the teeth under the Geneva 2000 for distribution in the US and Canada. In the same year he established the Geneva Dental Institute which provided education on the Geneva 2000 Prosthetic system. The same system, using the same tools Dr. Frush developed over 20 years ago. Throughout the 1980s, in the United Kingdom the Swissedent system was used as the only system that had continuity between Dentists and Dental Technicians training in prosthetics and was used in many dental schools. It was the only system that had different training protocols for Dentists and Dental Technicians when added together created natural looking dentures. In 2010, Mr. Kashif Qureshi a qualified Dental Technician who had trained on the Swissedent system, as an apprentice was applying to become a Clinical Dental Technician (Denturists) and open a Denture Clinic with the Swissedent name. Between 2013 – 2015, Mr.Kashif Qureshi trained to become a Clinical Dental Technician, utilising all of the knowledge from the Swissedent system from the technical and clinical (Dentist & Dental Technician training system) aspect of Swissedent Dentures . In 2015, Mr. Kashif Qureshi, a graduate from the University of Central Lancashire, opened the Swissedent Denture Clinic to treat patients for 'Natural Looking Dentures' from his combined knowledge of the technical and clinical aspects of the Swissedent system. From 700 BCE to the breakthrough of natural looking dentures in 1951, the history of dentures will continue to live on. What will be next in our denture history? The launch of the NHS in 1948 meant, for the first time-ever, that dental care was free at the point of use, dramatically changing people's access to good oral healthcare, their expectations, and their appreciation of looking after their oral health. The introduction of the NHS in 1948 gave the British population free access to dental treatment. There was a school dental service and a special priority service for expectant and nursing mothers, and young children that was organised by local authorities. However there was such a demand for dentures, nicknamed the dash for dentures, that a far higher proportion of the budget was spent on this than anticipated. The poor state of British teeth had been highlighted at the end of the previous century by the British Army's recruits for the Boer War: of 208,300, there were 6,942 hospital admissions owing to dental causes, of which one third had to be sent home unfit to serve. In 1948 the nation's dental health was in a worse state than that of defeated and occupied Germany: decay, pyorrhoea, and sepsis were rife. More than three quarters of the population over the age of 18 had complete dentures. When the NHS opened for business on 5 July 1948, we estimate that just over a quarter of practising dentists had signed up to work in the NHS. The demand for dental care on the new NHS was overwhelming. Dentists went from seeing around 15 to 20 patients a day to over 100. Patients had to be turned away, and hospitals also experienced a rise in cases. In the first nine months of its existence NHS dentists provided over 33 million artificial teeth, a figure that would rise to 65.5 million for the year 1950-1951. By 1951, the NHS was already running out of money. To help alleviate this, charges for dentures, the first charges of any kind for NHS treatment, were introduced causing much debate in government and the public arena and leading to the resignation of Aneurin Bevan, the Minister who had been crucial to bringing the NHS into existence. Article by BDA, The story of NHS Dentistry, accessed 18th April 2020)  Click below for the 'The History of Natural Looking Dentures':
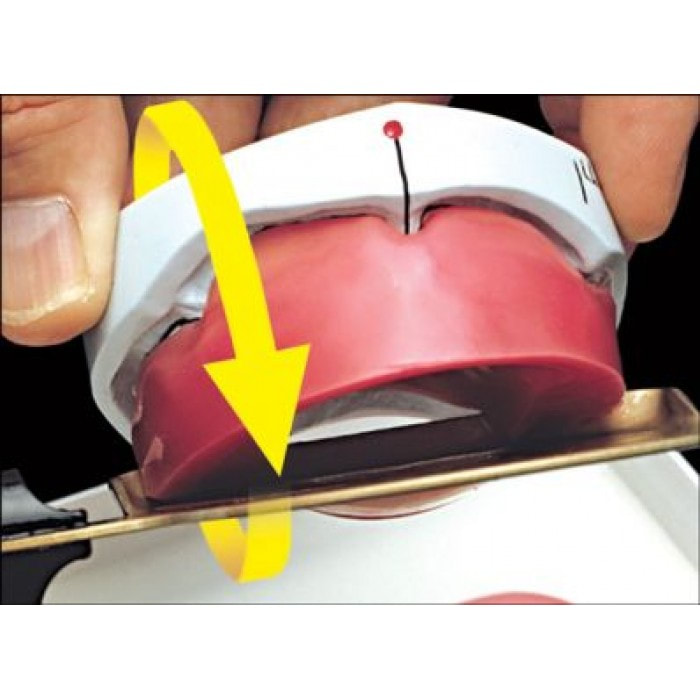
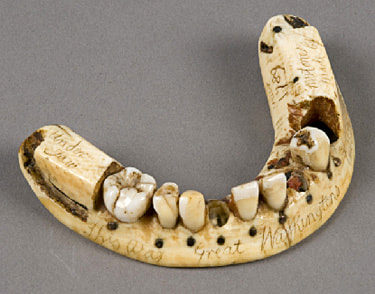
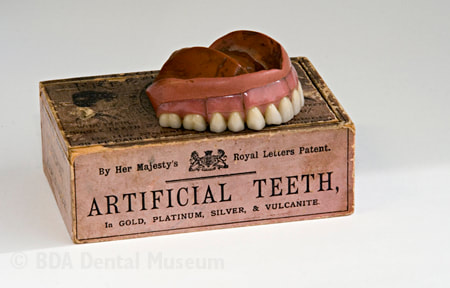
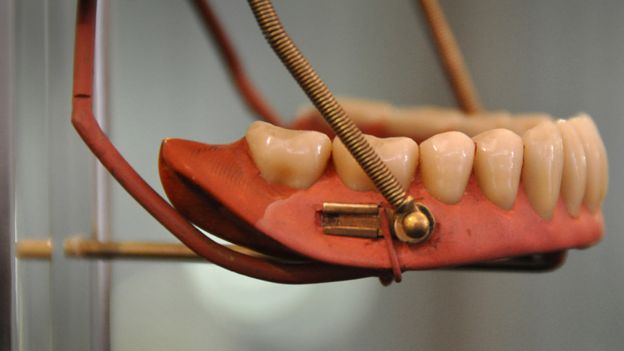
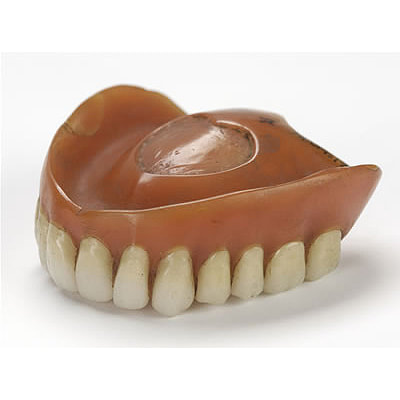
The History Of Dentures – Time Line From 700 BCE Year 700 BC The first set of Dentures was made by Etruscan people living in Etruria (Umbria and Tuscany, Italy) from 700 BC onwards. Teeth was used from other humans or animals and was inserted and pinned together via a gold band with a metal pin and fitted onto the remaining teeth, this option was expensive and only for the wealthy. (Figure 1, 2 Copy of an Etruscan denture, Science Museum London) Year 1600 In the early 1600s: Japan invented the first set of functional complete dentures out of wood (Figure 2) but later versions introduced the use of ivory, animal horns sculpted to mimic natural teeth. Animal's such as the hippopotamus and elephant ivory was carved into dentures to imitate natural teeth. Over time, the ivory became stained and gave off a foul smell and were uncomfortable to wear. Full lower sets were weighted to help gravity. To help upper sets stay in place springs were attached to the bottom set and the spring thus pushed the upper set upwards. (Figure 3, 4 BDA Dental Museum) Year 1700 In the 1700's: John Hunter, attempted to transplant human teeth into a comb of a rooster. Studies showed this was unsuccessful although the tooth was firmly implanted in the rooster, it did not work for humans. Although it was considered unsuccessful it created principles for future implantation. Around the 1770s, Alexis Duchâtea created the first set of porcelain dentures. (Figure 5, source unknown) Year 1800 In the early 1800s: A major source of teeth was scavenged from dead soldiers in the battle fields of Europe following the Battle of Waterloo. In 1815, dentures was constructed with the teeth of the dead soldiers and was known as ‘Waterloo Teeth’ and fixed onto a ivory base. (Figure 8 -12 BDA Dental Museum) They would have been shaped and sorted to make it look like each set of upper and lower front teeth had come from a single body. The sets would have been sold to early dental technicians who would boil them, chop off the ends, and then shape them on to ivory dentures. (Figure 13, BDA Dental Museum) Year 1820 In 1820: English goldsmith and dental manufacturer Claudius Ash mounted porcelain on 18-karat gold plates, with gold springs and swivels. (Figure 14, unknown source) Year 1840 - 1850 In the 1840s - 1850s: The Goodyear family invented and developed a material that was used for the bases of dentures called Vulcanite. This material would replace the ivory in previous dentures with a hardened rubber material . The properties of Vulcanite allowed the material to be easily mouldable to a humans gums and harden without losing the shape of the gums. This was considered a cheaper option than gold denture bases which made dentures affordable for everyone. (Figure 15 - 19 BDA Dental Museum) Year 1851 In 1851: Edwin Truman used Gutta Percha material as a replacement for Vulcanite but later found the material was unstable and needed complicated equipment. (Figure 20, unknown source) Year 1868 In 1868:John Hayatt discovered a substitute material for Vulcanite called Celluloid, this was unsuccessful due to its absorption of stains, odours and the dentures colour changing to a black colour and being highly flammable as it used camphor as a plasticizer. (Figure 21, unknown source) Year 1901 In 1901: Dr. Otto Rohn prepared studies on a new material called poly methyl methacrylate. Year 1909 In 1909 Dr. Leo Bakeland discovered phenol-formaldehyde resin (bakelite) but was unsuccessful due its unstable dimensional properties and lack of uniformity, this was used in dentistry from 1924 and 1939. Year 1937 In 1937 Dr. Walter H Wright presented the studies of the use of poly methyl methacrylate resin as a denture base to the National Society of Denture Prosthetics in America. Year 1938 - present From 1938 polymethylmethacylite (PMMA or acrylic resin) became prevailing material for denture base and acrylic teeth. It is hard, translucent and inert (has no unpleasant odor or toxicity), it can be easily repaired and it is inexpensive. The acrylic teeth and denture base chemically and mechanically bond together to provide a stable denture with excellent properties. PMMA acrylic teeth are available variety of shades, shapes moulds to create a unique, realistic denture, which allow the ‘Dental Professional’ to create a functional, natural looking denture unique to the patient. (Figure 22, Metrodent, Candulor) PMMA denture base comes in a variety of shades to realistically match the pigment of the gingiva with high flexural strength properties (Figure 23, Diamond D, Keystone Industries). Click below for the next part: ' The History of NHS Dentistry'
#dental #lab #dentistry #dental #laboratory #newsletter #dentist #dentallablondon #dentallaboratory #dentaltechnician #dentista #odontologia #teeth #health #healthcare #bremadent #london #digitaldentistry #cadcam #implants #prosthetics #dentures #crowns #orthodontics
|
Private Dental Laboratory in London
 Kash Qureshi - Managing Director, Clinical Dental Technician Kash Qureshi - Managing Director, Clinical Dental Technician
About the author:
Kash Qureshi is a Clinical Dental Technician (Denturist) in the U.K who oversees and quality controls over 3000+ fixed and removable prosthesis including implant cases from a clinical and technical aspect monthly at Bremadent Dental Laboratory & Swissedent Denture Clinic in London. www.swissedent.co.uk www.bremadent.co.uk office@bremadent.co.uk 
Categories
All
Archives
May 2024
|




























 RSS Feed
RSS Feed
Let's Keep Connected!
ADDRESS: 25A St James Street, London, E17 7PJ - PHONE: 0208 520 8528 - EMAIL: office@bremadent.co.uk